

Long-Term Prognostic Value of Myocardial Viability by Myocardial Contrast Echocardiography in Patients after Acute Myocardial Infarction: A Systematic Review and Meta-Analysis
- PMID: 36295589
- PMCID: PMC9611281
- DOI: 10.3390/medicina58101429
Long-Term Prognostic Value of Myocardial Viability by Myocardial Contrast Echocardiography in Patients after Acute Myocardial Infarction: A Systematic Review and Meta-Analysis
Abstract
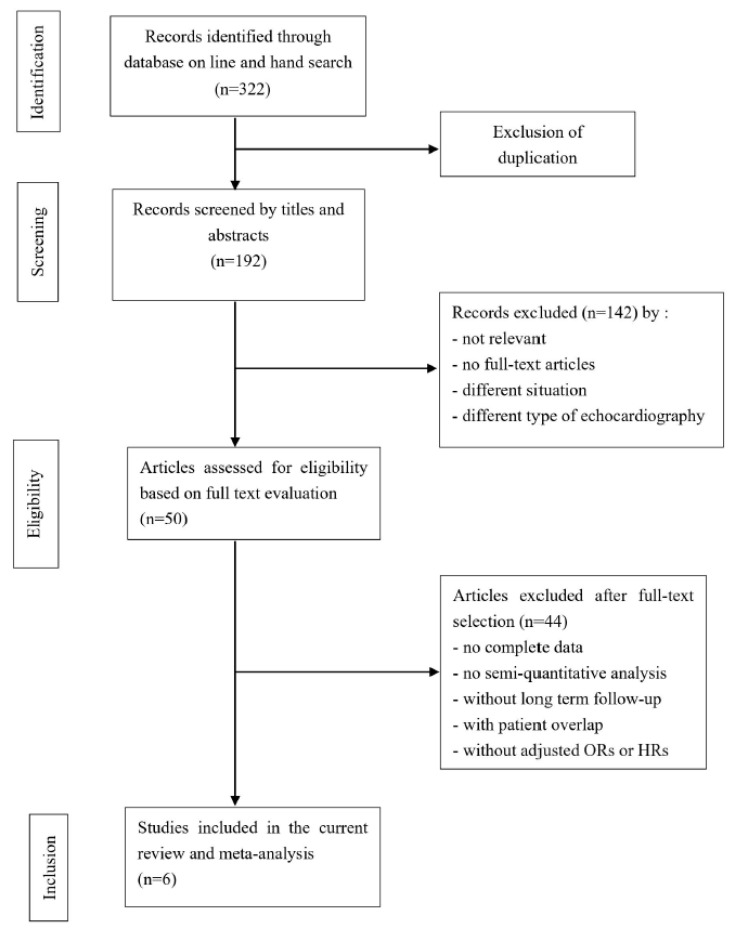
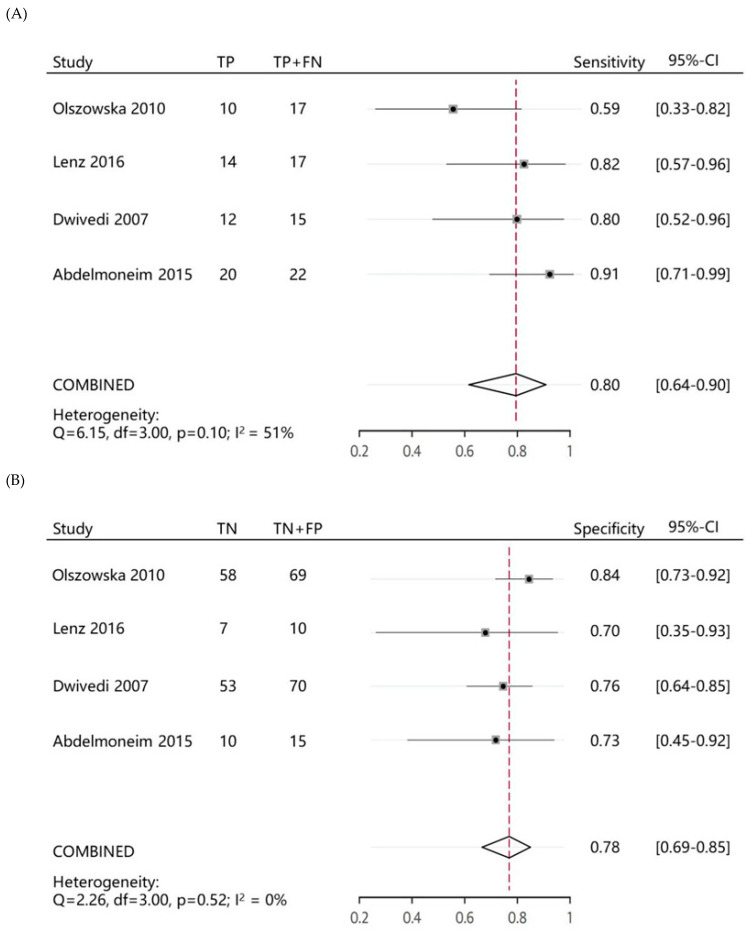
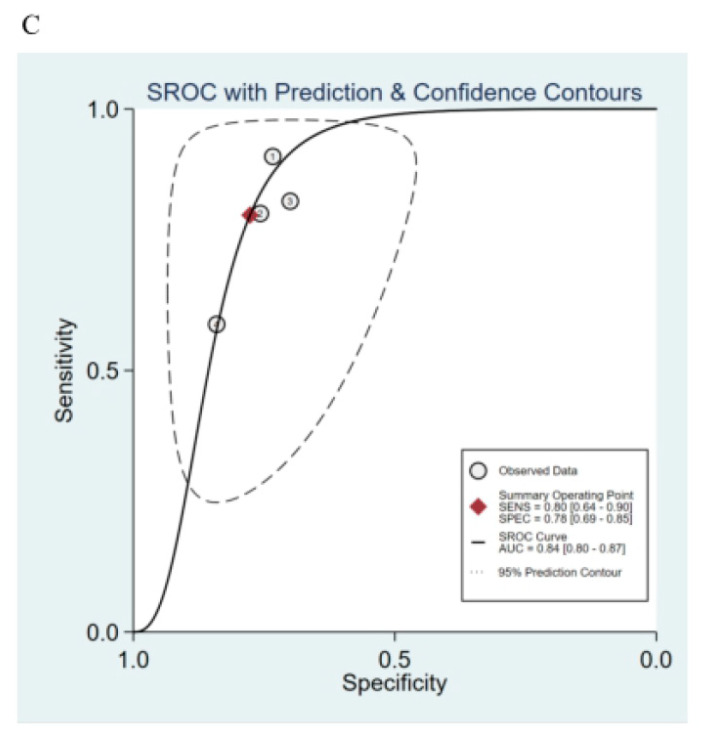
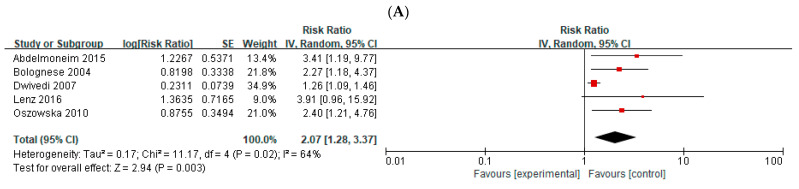
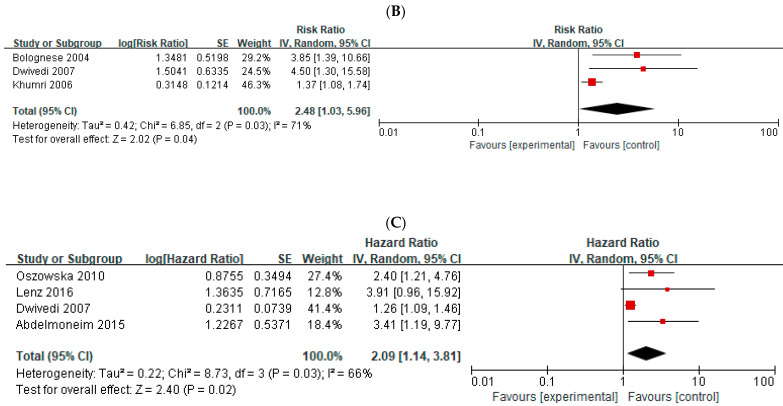
Background and Objectives: According to recent guidelines, myocardial contrast echocardiography (MCE) is recommended for detecting residual myocardial viability (MV). However, the long-term prognostic value of MV as assessed by MCE in identifying major adverse cardiac events (MACE) after acute myocardial infarction (AMI) remains undefined. Materials and Methods: We searched multiple databases, including PubMed, EMBASE, and Web of Science for studies on the prognostic value of MCE for clinical outcomes in AMI patients. The primary endpoints were MACEs during follow-up. Six studies that evaluated a total of 536 patients with a mean follow-up of 36.8 months were reviewed. Results: The pooled sensitivity and specificity of MCE for predicting MACEs were 0.80 and 0.78, respectively, and the summary operating receiver characteristics achieved an area under the curve of 0.84. The pooled relative risks demonstrated that the MV evaluated by MCE after AMI was correlated with a high risk for total cardiac events (pooled relative risk: 2.07; 95% confidence interval: 1.28-3.37) and cardiac death (pooled relative risk: 2.48; 95% confidence interval: 1.03-5.96). MV evaluated by MCE was a highly independent predictor of total cardiac events (pooled hazard ratio: 2.09, 95% confidence interval: 1.14-3.81) in patients after AMI. Conclusions: Residual MV evaluated by MCE may be an effective long-term prognostic tool for predicting MACE in patients after AMI that can provide moderate predictive accuracy. The assessment of MV by MCE may become an alternative technique with the potential to rapidly provide important information for improving long-term risk stratification in patients after AMI, at the bedside in clinical practice, especially for patients who cannot tolerate prolonged examinations. The PROSPERO registration number is CRD42020167565.
Keywords: acute myocardial infarction; meta-analysis; myocardial contrast echocardiography; myocardial viability; prognosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The comparative and added prognostic value of biomarkers to the Revised Cardiac Risk Index for preoperative prediction of major adverse cardiac events and all-cause mortality in patients who undergo noncardiac surgery.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD013139. doi: 10.1002/14651858.CD013139.pub2. Cochrane Database Syst Rev. 2021. PMID: 34931303 Free PMC article.
-
Beta-blockers in patients without heart failure after myocardial infarction.Cochrane Database Syst Rev. 2021 Nov 5;11(11):CD012565. doi: 10.1002/14651858.CD012565.pub2. Cochrane Database Syst Rev. 2021. PMID: 34739733 Free PMC article.
-
Myocardial contrast echocardiography evaluation of coronary microvascular dysfunction to Predict MACEs in patients with heart failure with preserved ejection fraction follow-up.BMC Cardiovasc Disord. 2024 Sep 18;24(1):496. doi: 10.1186/s12872-024-04173-7. BMC Cardiovasc Disord. 2024. PMID: 39289634 Free PMC article.
-
Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Feb 24;2(2):CD013556. doi: 10.1002/14651858.CD013556.pub2. Cochrane Database Syst Rev. 2022. PMID: 35199850 Free PMC article.
-
Exercise-based cardiac rehabilitation for coronary heart disease.Cochrane Database Syst Rev. 2021 Nov 6;11(11):CD001800. doi: 10.1002/14651858.CD001800.pub4. Cochrane Database Syst Rev. 2021. PMID: 34741536 Free PMC article.
Cited by
-
Low-dose dobutamine stress myocardial contrast echocardiography for evaluating myocardial microcirculation perfusion and predicting long-term prognosis in ST-segment elevation myocardial infarction after percutaneous coronary intervention.J Cardiothorac Surg. 2025 Feb 13;20(1):125. doi: 10.1186/s13019-024-03216-6. J Cardiothorac Surg. 2025. PMID: 39948581 Free PMC article.
References
-
- O’Gara P.T., Kushner F.G., Ascheim D.D., Casey D.E., Jr., Chung M.K., de Lemos J.A., Ettinger S.M., Fang J.C., Fesmire F.M., Franklin B.A., et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013;61:e78–e140. doi: 10.1016/j.jacc.2012.11.019. - DOI - PubMed
-
- Amier R.P., Smulders M.W., van der Flier W.M., Bekkers S.C.A.M., Zweerink A., Allaart C.P., Demirkiran A., Roos S.T., Teunissen P.F.A., Appelman Y., et al. Long-Term Prognostic Implications of Previous Silent Myocardial Infarction in Patients Presenting With Acute Myocardial Infarction. JACC Cardiovasc. Imaging. 2018;11:1773–1781. doi: 10.1016/j.jcmg.2018.02.009. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
