

Berberine Overcomes Gemcitabine-Associated Chemoresistance through Regulation of Rap1/PI3K-Akt Signaling in Pancreatic Ductal Adenocarcinoma
- PMID: 36297310
- PMCID: PMC9611392
- DOI: 10.3390/ph15101199
Berberine Overcomes Gemcitabine-Associated Chemoresistance through Regulation of Rap1/PI3K-Akt Signaling in Pancreatic Ductal Adenocarcinoma
Abstract
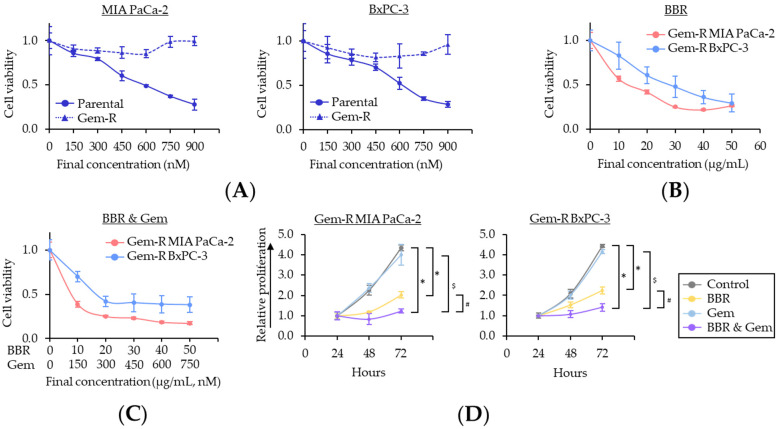
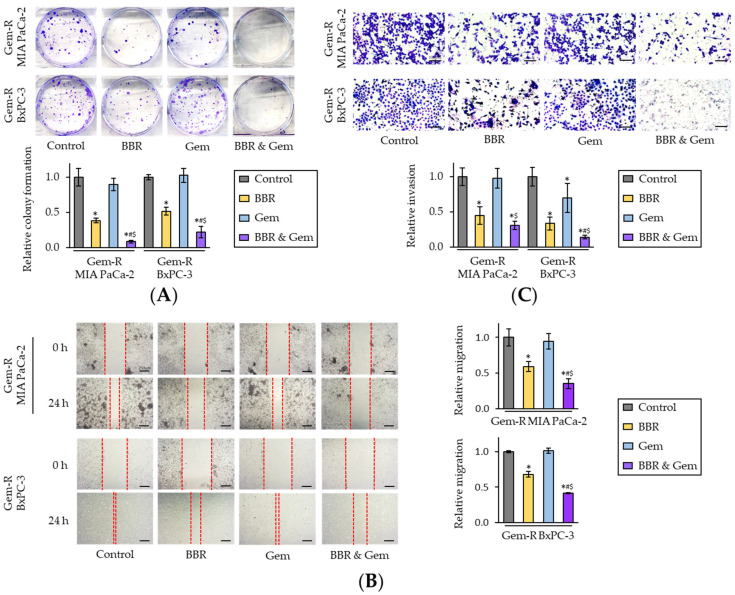
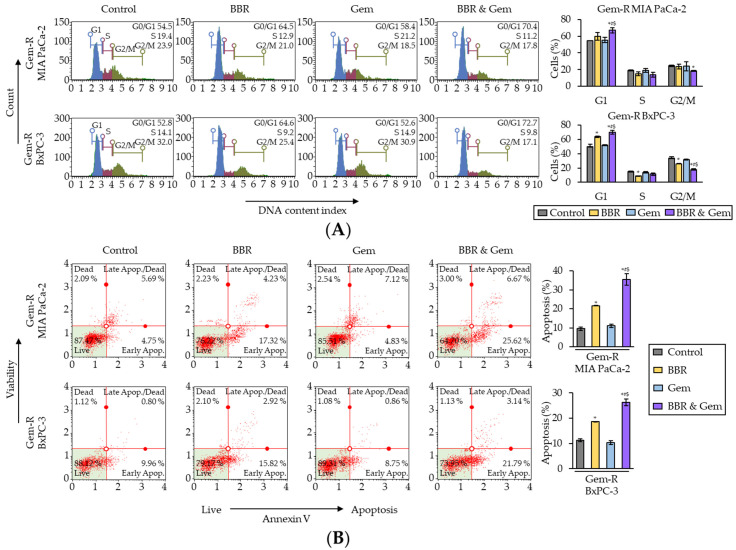
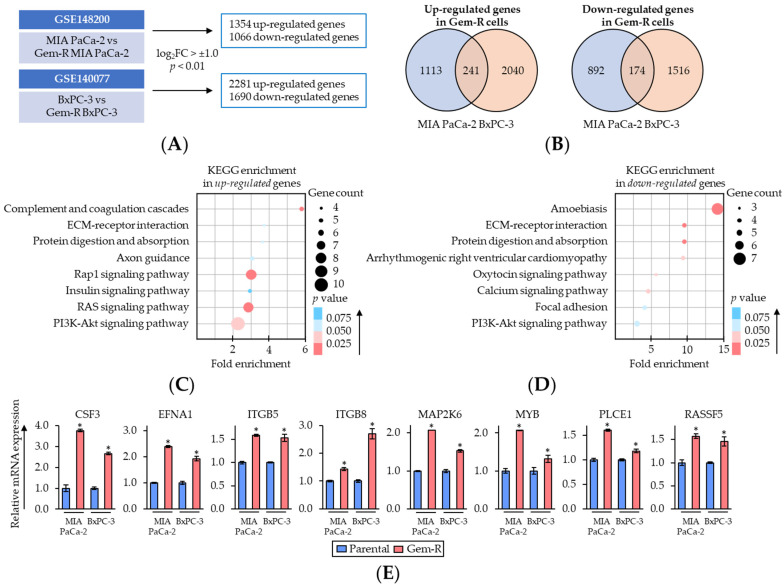
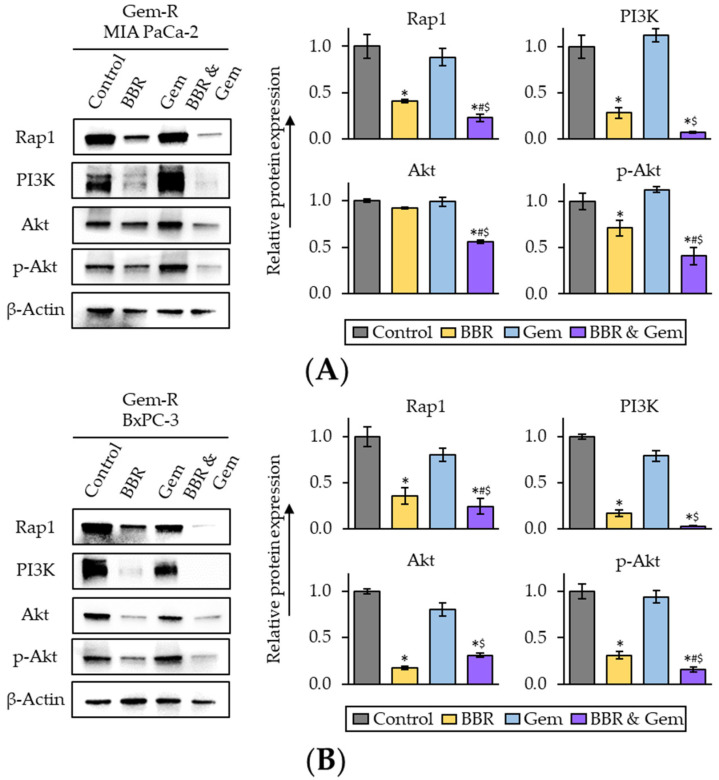
Gemcitabine (Gem)-based chemotherapy is one of the first-line treatments for pancreatic ductal adenocarcinoma (PDAC). However, its clinical effect is limited due to development of chemoresistance. Various naturally occurring compounds, including Berberine (BBR), provide an anti-cancer efficacy with time-tested safety, individually and in combination with chemotherapeutic drugs. Accordingly, we hypothesized that BBR might enhance the chemosensitivity to Gem in PDAC. In this study, cell culture studies using MIA PaCa-2 and BxPC-3 cells, followed by analysis in patient-derived organoids were performed to evaluate the anti-cancer effects of BBR in PDAC. Considering that cancer is a significant manifestation of increased chronic inflammatory stress, systems biology approaches are prudent for the identification of molecular pathways and networks responsible for phytochemical-induced anti-cancer activity, we used these approaches for BBR-mediated chemosensitization to Gem. Firstly, Gem-resistant (Gem-R) PDAC cells were established, and the combination of BBR and Gem revealed superior anti-cancer efficacy in Gem-R cells. Furthermore, the combination treatment induced cell cycle arrest and apoptosis in Gem-R PDAC cells. Transcriptomic profiling investigated the Rap1 and PI3K-Akt signaling pathway as a key regulator of Gem-resistance and was a key mediator for BBR-mediated chemosensitization in PDAC cells. All cell culture-based findings were successfully validated in patient-derived organoids. In conclusion, we demonstrate that BBR-mediated reversal of chemoresistance to Gem manifests through Rap1/PI3K-Akt signaling in PDAC.
Keywords: Berberine; Gemcitabine; Rap1/PI3K-Akt signaling pathway; chemoresistance; pancreatic ductal adenocarcinoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Andrographis Reverses Gemcitabine Resistance through Regulation of ERBB3 and Calcium Signaling Pathway in Pancreatic Ductal Adenocarcinoma.Biomedicines. 2023 Jan 3;11(1):119. doi: 10.3390/biomedicines11010119. Biomedicines. 2023. PMID: 36672630 Free PMC article.
-
Combination of RUNX1 inhibitor and gemcitabine mitigates chemo-resistance in pancreatic ductal adenocarcinoma by modulating BiP/PERK/eIF2α-axis-mediated endoplasmic reticulum stress.J Exp Clin Cancer Res. 2023 Sep 11;42(1):238. doi: 10.1186/s13046-023-02814-x. J Exp Clin Cancer Res. 2023. PMID: 37697370 Free PMC article.
-
TIMP1 down-regulation enhances gemcitabine sensitivity and reverses chemoresistance in pancreatic cancer.Biochem Pharmacol. 2021 Jul;189:114085. doi: 10.1016/j.bcp.2020.114085. Epub 2020 Jun 6. Biochem Pharmacol. 2021. PMID: 32522594
-
Brucein D augments the chemosensitivity of gemcitabine in pancreatic cancer via inhibiting the Nrf2 pathway.J Exp Clin Cancer Res. 2022 Mar 10;41(1):90. doi: 10.1186/s13046-022-02270-z. J Exp Clin Cancer Res. 2022. PMID: 35272669 Free PMC article.
-
Complex roles of the stroma in the intrinsic resistance to gemcitabine in pancreatic cancer: where we are and where we are going.Exp Mol Med. 2017 Dec 1;49(12):e406. doi: 10.1038/emm.2017.255. Exp Mol Med. 2017. PMID: 29611542 Free PMC article. Review.
Cited by
-
Curcumin-Mediated Resistance to Lenvatinib via EGFR Signaling Pathway in Hepatocellular Carcinoma.Cells. 2023 Feb 14;12(4):612. doi: 10.3390/cells12040612. Cells. 2023. PMID: 36831279 Free PMC article.
-
m6A eraser FTO impairs gemcitabine resistance in pancreatic cancer through influencing NEDD4 mRNA stability by regulating the PTEN/PI3K/AKT pathway.J Exp Clin Cancer Res. 2023 Aug 22;42(1):217. doi: 10.1186/s13046-023-02792-0. J Exp Clin Cancer Res. 2023. PMID: 37605223 Free PMC article.
-
The LAMB3-EGFR signaling pathway mediates synergistic Anti-Cancer effects of berberine and emodin in Pancreatic cancer.Biochem Pharmacol. 2024 Oct;228:116509. doi: 10.1016/j.bcp.2024.116509. Epub 2024 Aug 28. Biochem Pharmacol. 2024. PMID: 39214450
-
AUM302, a novel triple kinase PIM/PI3K/mTOR inhibitor, is a potent in vitro pancreatic cancer growth inhibitor.PLoS One. 2023 Nov 9;18(11):e0294065. doi: 10.1371/journal.pone.0294065. eCollection 2023. PLoS One. 2023. PMID: 37943821 Free PMC article.
-
Cholesterol neutralized vemurafenib treatment by promoting melanoma stem-like cells via its metabolite 27-hydroxycholesterol.Cell Mol Life Sci. 2024 May 22;81(1):226. doi: 10.1007/s00018-024-05267-3. Cell Mol Life Sci. 2024. PMID: 38775844 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
