

Potential vestibular pathway impairment in children with recurrent vertigo: An investigation through air-conducted sound and galvanic vestibular stimulation-triggered vestibular evoked myogenic potentials
- PMID: 36299274
- PMCID: PMC9588909
- DOI: 10.3389/fneur.2022.997205
Potential vestibular pathway impairment in children with recurrent vertigo: An investigation through air-conducted sound and galvanic vestibular stimulation-triggered vestibular evoked myogenic potentials
Abstract
Objective: This study aims to investigate the potential vestibular pathway impairment through vestibular evoked myogenic potentials (VEMPs) and to explore the pathophysiological significance of these instrument-based findings in children with recurrent vertigo.
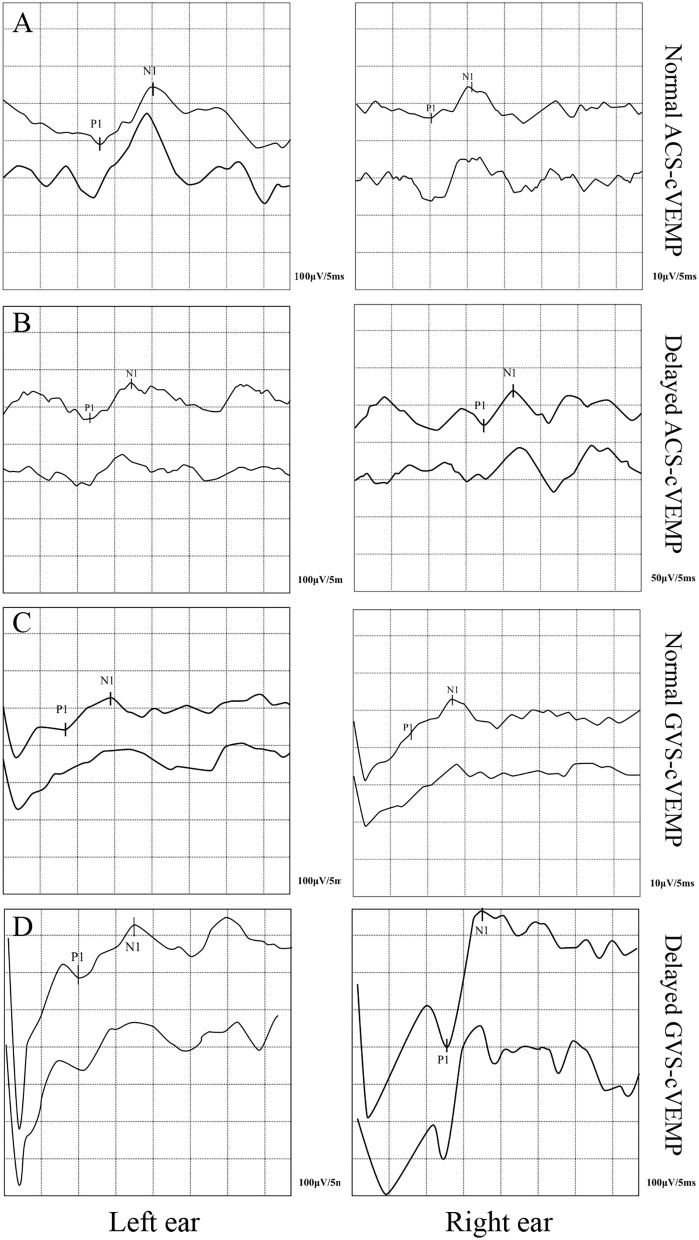
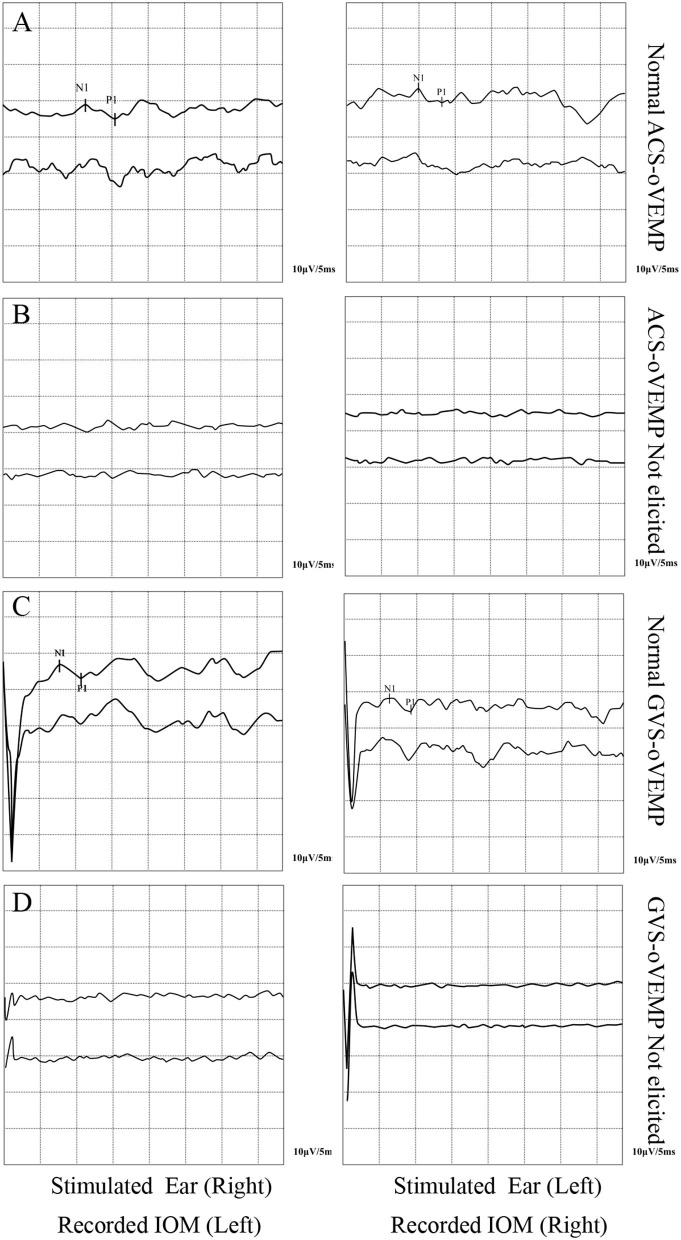
Materials and methods: The clinical data of 21 children (mean age 4.67 ± 1.39 years) diagnosed as RVC who met the inclusion criteria of the Bárány Society and 29 healthy children (mean age 4.83 ± 1.34 years) enrolled as the control group from February 2021 to December 2021 were collected and analyzed retrospectively. All the subjects underwent both cervical VEMP (cVEMP) and ocular VEMP (oVEMP) triggered by air-conducted sound (ACS) and galvanic vestibular stimulation (GVS), respectively. The elicit rate, latency, and amplitude asymmetry ratio (AAR) of ACS-cVEMP, ACS-oVEMP, GVS-cVEMP, and GVS-oVEMP were analyzed.
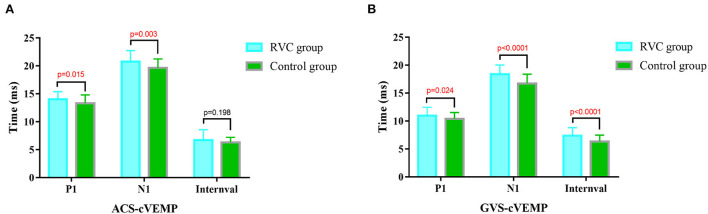
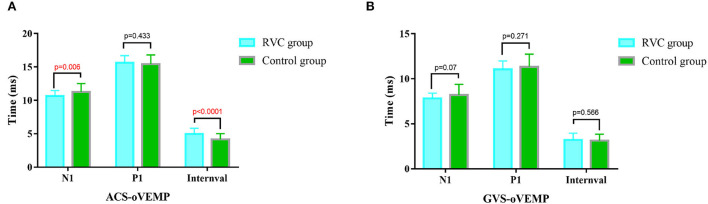
Results: (1) The elicit rates of ACS-cVEMP and ACS-oVEMP were similar in the two groups (P > 0.05), as well as GVS-cVEMP and GVS-oVEMP (P > 0.05). (2) P1 and N1 latencies of ACS-cVEMP and GVS-cVEMP in the RVC group were longer than those in the control group (P < 0.05). (3) The N1 latency of ACS-oVEMP in the RVC group was shorter than that in the control group (P < 0.05), while there was no significant difference in the P1 latency of ACS-oVEMP (P > 0.05). The N1 and P1 latencies of GVS-oVEMP were not significantly different (P > 0.05). (4) There was no statistical difference in the AAR of ACS-cVEMP and GVS-cVEMP. Although there was an increased AAR of ACS-oVEMP in the RVC group (P < 0.05), the AAR was within the normal range. However, no statistical difference was found in the AAR of GVS-oVEMP in the two groups (P > 0.05).
Conclusion: The latencies of ACS-cVEMP and GVS-cVEMP in children with recurrent vertigo were significantly prolonged compared with those in healthy children, and there was no difference in elicit rates of ACS-cVEMP and GVS-cVEMP, suggesting that there might be potential impairment in the inferior vestibular nerve and the subsequent nerve conduction pathway in RVC.
Keywords: elicit rate; latency; recurrent vertigo of childhood; saccule; utricle; vestibular evoked myogenic potential; vestibular pathway.
Copyright © 2022 Sun, Gao, Shen, Zhu, Wang, Ma, Wang, Chen, Zhang, Jin, Chen and Yang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical characteristics of vestibular evoked myogenic potentials in children with recurrent vertigo of childhood.Int J Pediatr Otorhinolaryngol. 2022 Oct;161:111257. doi: 10.1016/j.ijporl.2022.111257. Epub 2022 Aug 7. Int J Pediatr Otorhinolaryngol. 2022. PMID: 35988372
-
The functional status of vestibular otolith and conductive pathway in patients with unilateral idiopathic sudden sensorineural hearing loss.Front Neurol. 2023 Jul 20;14:1237516. doi: 10.3389/fneur.2023.1237516. eCollection 2023. Front Neurol. 2023. PMID: 37545733 Free PMC article.
-
[Preliminary observation of galvanic vestibular stimulation-vestibular evoked myogenic potentials in healthy young people].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019 Jun 7;54(6):432-438. doi: 10.3760/cma.j.issn.1673-0860.2019.06.007. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019. PMID: 31262108 Chinese.
-
Clinical significance of cervical and ocular vestibular evoked myogenic potentials in benign paroxysmal positional vertigo: a meta-analysis.Eur Arch Otorhinolaryngol. 2019 Dec;276(12):3257-3265. doi: 10.1007/s00405-019-05674-4. Epub 2019 Oct 11. Eur Arch Otorhinolaryngol. 2019. PMID: 31605189 Review.
-
Ocular vs. Cervical Vestibular Evoked Myogenic Potentials in Benign Paroxysmal Positional Vertigo: A Systematic Review and Meta-Analysis.Front Neurol. 2020 Oct 26;11:596454. doi: 10.3389/fneur.2020.596454. eCollection 2020. Front Neurol. 2020. PMID: 33193065 Free PMC article.
References
-
- van de Berg R, Widdershoven J, Bisdorff A, Evers S, Wiener-Vacher S, Cushing SL, et al. . Vestibular migraine of childhood and recurrent vertigo of childhood: diagnostic criteria consensus document of the committee for the classification of vestibular disorders of the bárány society and the international headache society. J Vestib Res. (2021) 31:1–9. 10.3233/VES-200003 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous