

Haemodynamic effects of initial combination therapy in pulmonary arterial hypertension: a systematic review and meta-analysis
- PMID: 36299361
- PMCID: PMC9589336
- DOI: 10.1183/23120541.00313-2022
Haemodynamic effects of initial combination therapy in pulmonary arterial hypertension: a systematic review and meta-analysis
Abstract
Background: Although the initial use of combination treatment has been proven to be beneficial for patients' clinical outcomes, there are scarce data on its haemodynamic effects. The objective of the present study was to evaluate the effect of an initial combination of pulmonary arterial hypertension (PAH)-targeted therapies on haemodynamic parameters in treatment-naïve PAH patients.
Methods: A systematic search of PubMed, Cochrane Central Register of Controlled Trials and Web of Science was performed. We considered eligible studies with an intervention of initial PAH-targeted combination therapy in treatment-naïve PAH patients with or without monotherapy control. A random-effects meta-analysis was performed for the difference between baseline and follow-up in pulmonary vascular resistance (PVR) and other haemodynamic parameters.
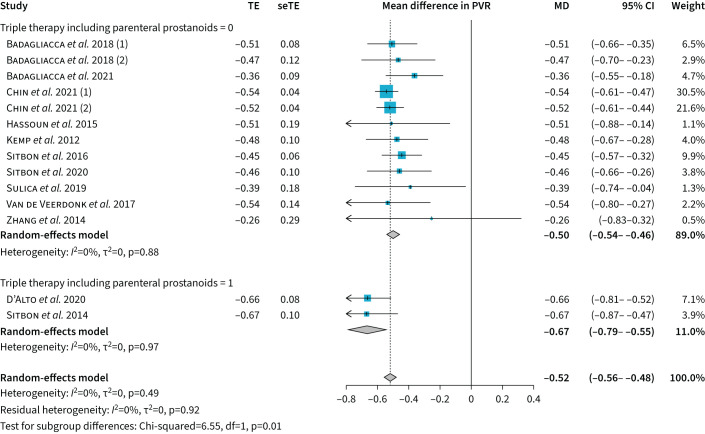
Results: In 880 patients receiving initial combination therapy PVR was reduced by -6.5 Wood Units (95% CI -7.4--5.7 Wood Units) or by -52% (95% CI -56%--48%, I2=0%) compared to baseline. Initial triple therapy including a parenteral prostanoid resulted in significantly greater PVR reduction (-67% versus -50% with all other combination therapies, p=0.01). The effect was more pronounced in younger patients (p=0.02). Compared to baseline, there was -12.2 mmHg (95% CI -14.0--10.4 mmHg) decrease in mean pulmonary artery pressure, 0.9 L·min-1·m-2 (95% CI 0.8-1.1 L·min-1·m-2) increase in cardiac index, -3.2 mmHg (95% CI -4.1--2.3 mmHg) decrease in right atrial pressure and 8.6% (95% CI 6.9-10.3%) increase in mixed venous oxygen saturation. In the controlled studies, initial combination therapy reduced PVR by -4.2 Wood Units (95% CI -6.1--2.4 Wood Units) compared to monotherapy.
Conclusion: Initial combination therapy leads to remarkable haemodynamic amelioration. Parenteral prostanoids should be considered early, especially in more severely affected patients, to enable right ventricular reverse remodelling.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: I.T. Farmakis has nothing to disclose. Conflict of interest: E. Vrana has nothing to disclose. Conflict of interest: S-A. Mouratoglou has nothing to disclose. Conflict of interest: S. Zafeiropoulos has nothing to disclose. Conflict of interest: S. Zanos has nothing to disclose. Conflict of interest: G. Giannakoulas has received fees for lectures and/or consultation from Actelion, Bayer, ELPEN Pharmaceuticals, GlaxoSmithKline, Janssen, MSD, Pfizer, Lilly and United Therapeutics.
Figures


References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous