

Procalcitonin and C-reactive protein in the diagnosis of spontaneous bacterial peritonitis
- PMID: 36300145
- PMCID: PMC9468983
- DOI: 10.21037/tgh-19-297
Procalcitonin and C-reactive protein in the diagnosis of spontaneous bacterial peritonitis
Abstract
Background: Spontaneous bacterial peritonitis (SBP) is a serious complication of cirrhosis and is associated with high morbidity and mortality. Rapid institution of appropriate antibiotics is central to the improved patient outcome. Correctly obtaining ascites fluid for analysis has several technical and logistic limitations resulting in overuse of empiric antibiotics when patients are admitted to the hospital with suspected SBP. Procalcitonin and C-reactive protein (CRP) are non-invasive markers of infection. We conducted a study to illustrate the role of these markers in making the diagnosis of SBP in patients with cirrhosis.
Methods: A total of 45 patients were enrolled in this prospective cohort study, 14 (31.1%) of which were found to have SBP. Ascitic fluid neutrophils, serum procalcitonin and CRP levels were measured prior to initiation of antibiotics and these parameters were compared between the two groups. Area under receiver operator characteristic (AUROC) curves were used to assess the diagnostic accuracy of procalcitonin and CRP in this population. We defined neutrocytic SBP group as a combination of patients who had classic SBP (positive ascitic culture and >250 neutrophils/mm3) and culture-negative neutrocytic ascites.
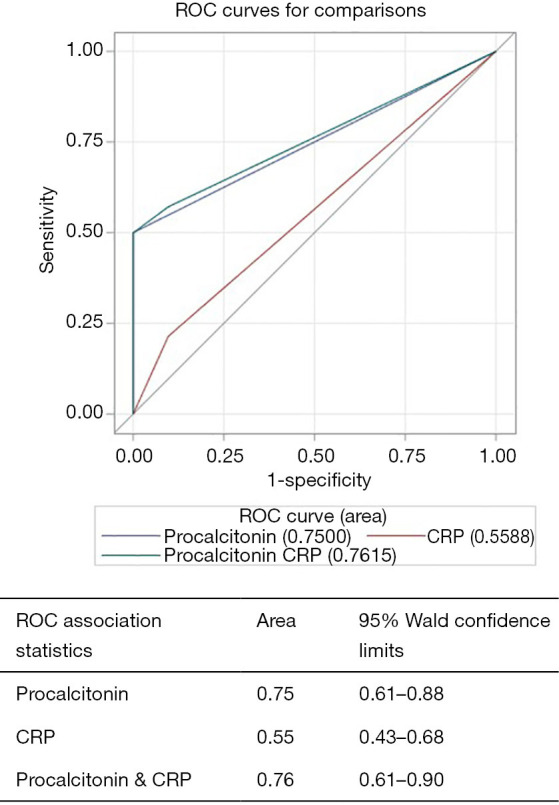
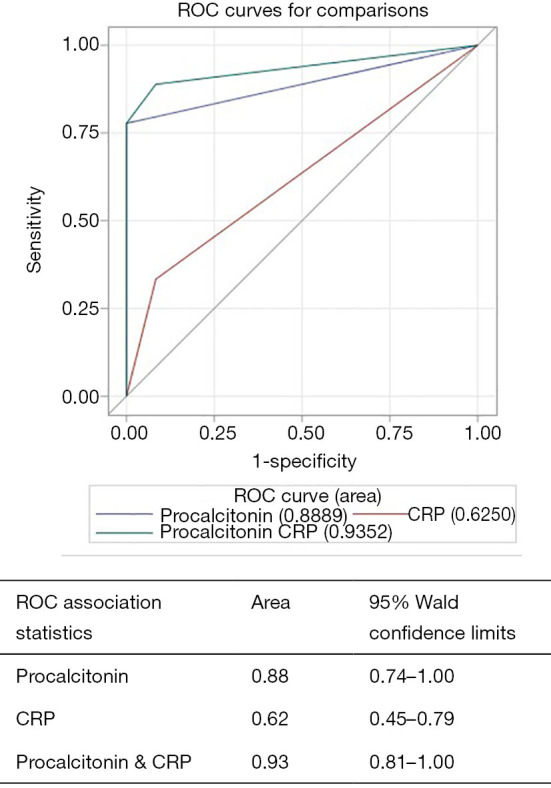
Results: Serum procalcitonin (2.81±2.59 vs. 0.43±0.48 ng/mL; P=0.0032), serum CRP (60.30±44.48 vs. 22.2±23.28; P=0.0055) and ascitic fluid neutrophil levels (49.23±30.90 vs. 16.7±20.39; P=0.0064) were significantly higher in SBP group than non-SBP group. AUROC for procalcitonin (cut-off >2.0 ng/mL) was 0.75 (95% CI, 0.61-0.88), CRP (cut-off >3.0 mg/L) was 0.55 (95% CI, 0.43-0.68) and for procalcitonin combined with CRP was 0.76 (95% CI, 0.61-0.90) for diagnosing all-cause SBP. In a subgroup analysis of patients with neutrocytic SBP, AUROC for procalcitonin was 0.88 (95% CI, 0.74-1.00), CRP was 0.62 (95% CI, 0.45-0.79) and for procalcitonin combined with CRP was 0.93 (95% CI, 0.81-1.00). Addition of CRP to procalcitonin did not significantly change the AUROC for diagnosis of SBP.
Conclusions: Serum procalcitonin could be used as an adjunctive non-invasive biomarker in diagnosing SBP with a high degree of accuracy in cirrhotic patients. Addition of CRP does not seem to significantly increase the diagnostic accuracy of procalcitonin.
Keywords: C-reactive protein (CRP); Procalcitonin; diagnosis; liver cirrhosis; peritonitis.
2022 Translational Gastroenterology and Hepatology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tgh.amegroups.com/article/view/10.21037/tgh-19-297/coif). SKS reports grants from Gilead Sciences, Conatus Pharma, Intercept Pharma, Genfit, Bayer, Exact Sciences, Biotest, Shire NASH and Enanta, outside the submitted work; he reports Speaker’s Bureau from Intercept Pharma, Alexion and Dova, outside the submitted work; he is on Advisory Board of Bayer and Biotest, outside the submitted work. SKS serves as an Editor-in-Chief of Translational Gastroenterology and Hepatology. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
The role of serum procalcitonin levels in predicting ascitic fluid infection in hospitalized cirrhotic and non-cirrhotic patients.Int J Med Sci. 2013 Aug 20;10(10):1367-74. doi: 10.7150/ijms.6014. eCollection 2013. Int J Med Sci. 2013. PMID: 23983598 Free PMC article.
-
The role of serum procalcitonin and C-reactive protein levels in predicting spontaneous bacterial peritonitis in patients with advanced liver cirrhosis.Pak J Med Sci. 2016 Nov-Dec;32(6):1484-1488. doi: 10.12669/pjms.326.10995. Pak J Med Sci. 2016. PMID: 28083050 Free PMC article.
-
Combination of PCT, sNFI and dCHC for the diagnosis of ascites infection in cirrhotic patients.BMC Infect Dis. 2018 Aug 10;18(1):389. doi: 10.1186/s12879-018-3308-1. BMC Infect Dis. 2018. PMID: 30097024 Free PMC article.
-
Value of serum procalcitonin levels in predicting spontaneous bacterial peritonitis.Hepatogastroenterology. 2013 Jun;60(124):641-6. doi: 10.5754/hge12645. Hepatogastroenterology. 2013. PMID: 23159389 Review.
-
Spontaneous bacterial peritonitis.Dis Mon. 1985 Sep;31(9):1-48. doi: 10.1016/0011-5029(85)90002-1. Dis Mon. 1985. PMID: 3899555 Review.
Cited by
-
Comparison of the Diagnostic Accuracies of Procalcitonin and C-Reactive Protein for Spontaneous Bacterial Peritonitis in Patients with Cirrhosis: A Systematic Review and Meta-Analysis.Medicina (Kaunas). 2025 Jun 24;61(7):1134. doi: 10.3390/medicina61071134. Medicina (Kaunas). 2025. PMID: 40731765 Free PMC article.
-
Predictors and Outcomes of Infections in ICU Patients With Cirrhosis: A Single-Center Observational Study.Cureus. 2023 Oct 16;15(10):e47151. doi: 10.7759/cureus.47151. eCollection 2023 Oct. Cureus. 2023. PMID: 38022175 Free PMC article.
-
Exploring the next frontier in diagnosing spontaneous bacterial peritonitis.World J Hepatol. 2025 Mar 27;17(3):102044. doi: 10.4254/wjh.v17.i3.102044. World J Hepatol. 2025. PMID: 40177199 Free PMC article.
-
Mid-regional pro-adrenomedullin: A rapid sepsis biomarker for diagnosing spontaneous bacterial peritonitis in cirrhosis.Eur J Clin Invest. 2025 Jun;55(6):e70021. doi: 10.1111/eci.70021. Epub 2025 Mar 7. Eur J Clin Invest. 2025. PMID: 40052388 Free PMC article.
-
Predictive Factors and Nomogram for Spontaneous Bacterial Peritonitis in Decompensated Cirrhosis Among the Elderly.J Inflamm Res. 2024 Dec 12;17:10901-10911. doi: 10.2147/JIR.S484629. eCollection 2024. J Inflamm Res. 2024. PMID: 39687773 Free PMC article.
References
-
- Thuluvath PJ, Morss S, Thompson R. Spontaneous bacterial peritonitis--in-hospital mortality, predictors of survival, and health care costs from 1988 to 1998. Am J Gastroenterol 2001;96:1232-6. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous