

Exploration of prognostic factors for prediction of mortality in elderly CAP population using a nomogram model
- PMID: 36300178
- PMCID: PMC9588947
- DOI: 10.3389/fmed.2022.976148
Exploration of prognostic factors for prediction of mortality in elderly CAP population using a nomogram model
Abstract
Background: The incidence and mortality rate of community-acquired pneumonia (CAP) in elderly patients were higher than the younger population. The assessment tools including CURB-65 and qSOFA have been applied in early detection of high-risk patients with CAP. However, several disadvantages exist to limit the efficiency of these tools for accurate assessment in elderly CAP. Therefore, we aimed to explore a more comprehensive tool to predict mortality in elderly CAP population by establishing a nomogram model.
Methods: We retrospectively analyzed elderly patients with CAP in Minhang Hospital, Fudan University. The least absolute shrinkage and selection operator (LASSO) logistic regression combined with multivariate analyses were used to select independent predictive factors and established nomogram models via R software. Calibration plots, decision curve analysis (DCA) and receiver operating characteristic curve (ROC) were generated to assess predictive performance.
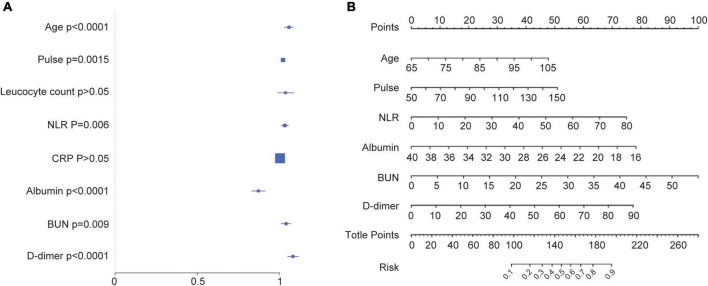
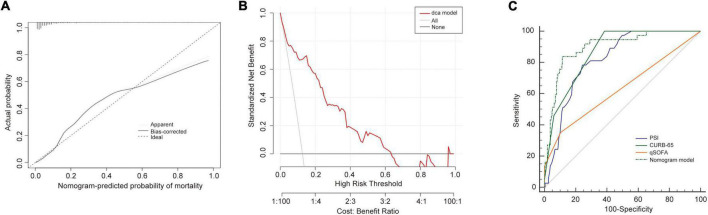
Results: LASSO and multiple logistic regression analyses showed the age, pulse, NLR, albumin, BUN, and D-dimer were independent risk predictors. A nomogram model (NB-DAPA model) was established for predicting mortality of CAP in elderly patients. In both training and validation set, the area under the curve (AUC) of the NB-DAPA model showed superiority than CURB-65 and qSOFA. Meanwhile, DCA revealed that the predictive model had significant net benefits for most threshold probabilities.
Conclusion: Our established NB-DAPA nomogram model is a simple and accurate tool for predicting in-hospital mortality of CAP, adapted for patients aged 65 years and above. The predictive performance of the NB-DAPA model was better than PSI, CURB-65 and qSOFA.
Keywords: CAP in elderly patients; CURB-65; nomogram model; prognosis; qSOFA.
Copyright © 2022 Lv, Li, Shi, Pan, Muhith, Peng, Xu and Deng.
Conflict of interest statement
Author WP was employed by Hunan Zixing Artificial Intelligence Technology Group Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




Similar articles
-
Establishment of risk model for elderly CAP at different age stages: a single-center retrospective observational study.Sci Rep. 2023 Aug 1;13(1):12432. doi: 10.1038/s41598-023-39542-3. Sci Rep. 2023. PMID: 37528213 Free PMC article.
-
Comparison of Different Scoring Systems for Prediction of Mortality and ICU Admission in Elderly CAP Population.Clin Interv Aging. 2021 Oct 28;16:1917-1929. doi: 10.2147/CIA.S335315. eCollection 2021. Clin Interv Aging. 2021. PMID: 34737556 Free PMC article.
-
A nomogram based on the expression level of angiopoietin-like 4 to predict the severity of community-acquired pneumonia.BMC Infect Dis. 2023 Oct 11;23(1):677. doi: 10.1186/s12879-023-08648-4. BMC Infect Dis. 2023. PMID: 37821811 Free PMC article.
-
Dynamic nomogram for predicting acute kidney injury in patients with community-acquired pneumonia.BMJ Open Respir Res. 2023 Sep;10(1):e001495. doi: 10.1136/bmjresp-2022-001495. BMJ Open Respir Res. 2023. PMID: 37739457 Free PMC article.
-
Nomogram for prediction of severe community-acquired pneumonia development in diabetic patients: a multicenter study.BMC Pulm Med. 2022 Nov 7;22(1):403. doi: 10.1186/s12890-022-02183-9. BMC Pulm Med. 2022. PMID: 36344933 Free PMC article. Clinical Trial.
Cited by
-
Development and validation of a predictive model for 30-day mortality in patients with severe community-acquired pneumonia in intensive care units.Front Med (Lausanne). 2024 Jan 8;10:1295423. doi: 10.3389/fmed.2023.1295423. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38259861 Free PMC article.
-
Establishment of risk model for elderly CAP at different age stages: a single-center retrospective observational study.Sci Rep. 2023 Aug 1;13(1):12432. doi: 10.1038/s41598-023-39542-3. Sci Rep. 2023. PMID: 37528213 Free PMC article.
-
Development and validation of a predictive model for hospital mortality in patients with community-acquired pneumonia admitted to the intensive care unit.J Int Med Res. 2025 May;53(5):3000605251340304. doi: 10.1177/03000605251340304. Epub 2025 May 23. J Int Med Res. 2025. PMID: 40406909 Free PMC article.
-
Development and application of a nomogram model for the prediction of carbapenem-resistant Klebsiella pneumoniae infection in neuro-ICU patients.Microbiol Spectr. 2024 Jan 11;12(1):e0309623. doi: 10.1128/spectrum.03096-23. Epub 2023 Dec 7. Microbiol Spectr. 2024. PMID: 38059625 Free PMC article.
-
Community-acquired Pneumonia among Elderly Patients Admitted to the Department of Medicine in a Tertiary Care Centre: A Descriptive Cross-sectional Study.JNMA J Nepal Med Assoc. 2023 Jun 1;61(262):535-538. doi: 10.31729/jnma.8202. JNMA J Nepal Med Assoc. 2023. PMID: 37464841 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous