

Factors associated with lesion detection in colonoscopy among different indications
- PMID: 36300971
- PMCID: PMC9731659
- DOI: 10.1002/ueg2.12325
Factors associated with lesion detection in colonoscopy among different indications
Abstract
Background and objective: Different factors may influence colonoscopy performance measures. We aimed to analyze procedure- and endoscopist-related factors associated with detection of colorectal lesions and whether these factors have a similar influence in the context of different colonoscopy indications: positive fecal immunochemical test (+FIT) and post-polypectomy surveillance colonoscopies.
Methods: This multicenter cross-sectional study included adults aged 40-80 years. Endoscopists (N = 96) who had performed ≥50 examinations were assessed for physician-related factors. Adenoma detection rate (ADR), adenomas per colonoscopy rate (APCR), advanced ADR, serrated polyp detection (SDR), and serrated polyps per colonoscopy rate (SPPCR) were calculated.
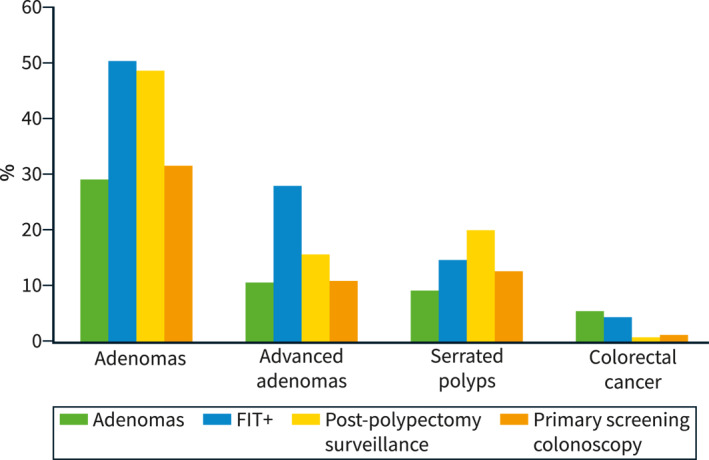
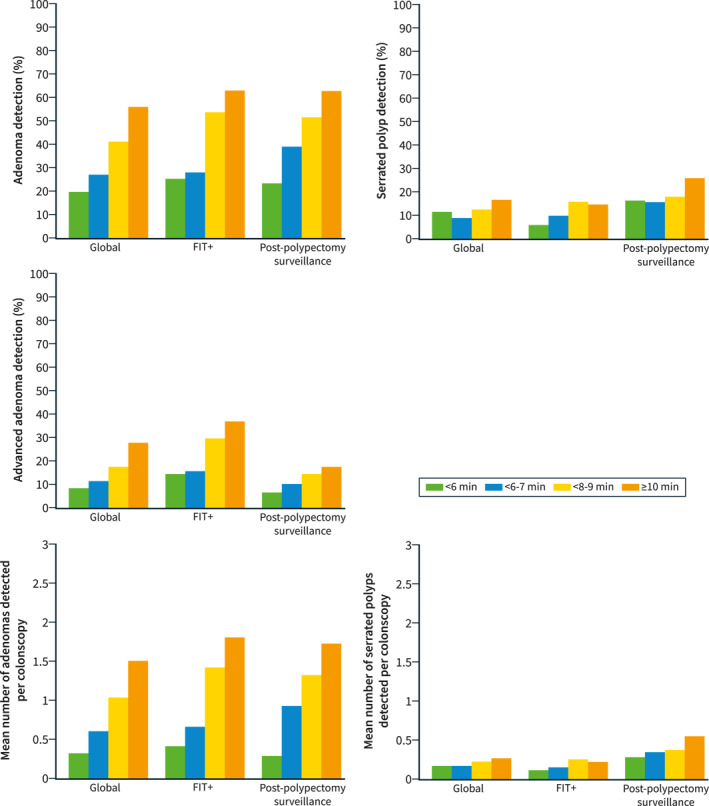
Results: We included 12,932 procedures, with 4810 carried out after a positive FIT and 1967 for surveillance. Of the 96 endoscopists evaluated, 43.8% were women, and the mean age was 41.9 years. The ADR, advanced ADR, and SDR were 39.7%, 17.7%, and 12.8%, respectively. Adenoma detection rate was higher in colonoscopies after a +FIT (50.3%) with a more than doubled advanced ADR compared to non-FIT procedures (27.6% vs. 13.0%) and similar results in serrated lesions (14.7% vs. 13.5%). Among all the detection indicators analyzed, withdrawal time was the only factor independently related to improvement (p < 0.001). Regarding FIT-positive and surveillance procedures, for both indications, withdrawal time was also the only factor associated with a higher detection of adenomas and serrated polyps (p < 0.001). Endoscopist-related factors (i.e., weekly hours dedicated to endoscopy, annual colonoscopy volume and lifetime number of colonoscopies performed) had also impact on lesion detection (APCR, advanced ADR and SPPCR).
Conclusions: Withdrawal time was the factor most commonly associated with improved detection of colonic lesions globally and in endoscopies for + FIT and post-polypectomy surveillance. Physician-related factors may help to address strategies to support training and service provision. Our results can be used for establishing future benchmarking and quality improvement in different colonoscopy indications.
Keywords: adenoma detection; colonoscopy; colorectal cancer; endoscopist; serrated polyp.
© 2022 The Authors. United European Gastroenterology Journal published by Wiley Periodicals LLC on behalf of United European Gastroenterology.
Conflict of interest statement
The author declares that they have no conflict of interest.
Figures
Similar articles
-
Differences in detection rates of adenomas and serrated polyps in screening versus surveillance colonoscopies, based on the new hampshire colonoscopy registry.Clin Gastroenterol Hepatol. 2013 Oct;11(10):1308-12. doi: 10.1016/j.cgh.2013.04.042. Epub 2013 May 6. Clin Gastroenterol Hepatol. 2013. PMID: 23660415 Free PMC article.
-
Providing data for serrated polyp detection rate benchmarks: an analysis of the New Hampshire Colonoscopy Registry.Gastrointest Endosc. 2017 Jun;85(6):1188-1194. doi: 10.1016/j.gie.2017.01.020. Epub 2017 Jan 31. Gastrointest Endosc. 2017. PMID: 28153571 Free PMC article.
-
Difference in Physician- and Patient-Dependent Factors Contributing to Adenoma Detection Rate and Serrated Polyp Detection Rate.Dig Dis Sci. 2019 Dec;64(12):3579-3588. doi: 10.1007/s10620-019-05808-y. Epub 2019 Aug 30. Dig Dis Sci. 2019. PMID: 31471862
-
Training interventions to improve adenoma detection rates during colonoscopy: a systematic review and meta-analysis.Surg Endosc. 2020 Sep;34(9):3870-3882. doi: 10.1007/s00464-019-07153-7. Epub 2019 Oct 8. Surg Endosc. 2020. PMID: 31595401
-
Magnitude, Risk Factors, and Factors Associated With Adenoma Miss Rate of Tandem Colonoscopy: A Systematic Review and Meta-analysis.Gastroenterology. 2019 May;156(6):1661-1674.e11. doi: 10.1053/j.gastro.2019.01.260. Epub 2019 Feb 6. Gastroenterology. 2019. PMID: 30738046
Cited by
-
Optimizing surveillance in Lynch syndrome: lesion detection and comparative performance of different colonoscopy modalities-a systematic review and network meta-analysis.Int J Colorectal Dis. 2025 Aug 12;40(1):175. doi: 10.1007/s00384-025-04970-2. Int J Colorectal Dis. 2025. PMID: 40796702 Free PMC article.
-
Current and future implications of artificial intelligence in colonoscopy.Ann Gastroenterol. 2023 Mar-Apr;36(2):114-122. doi: 10.20524/aog.2023.0781. Epub 2023 Feb 3. Ann Gastroenterol. 2023. PMID: 36864946 Free PMC article. Review.
-
Colorectal tumor comorbidity is common in patients with duodenal tumors: Exploratory cross-sectional study.Endosc Int Open. 2024 Oct 28;12(10):E1206-E1213. doi: 10.1055/a-2341-9026. eCollection 2024 Oct. Endosc Int Open. 2024. PMID: 39474485 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
