

Distinct Mechanisms of Mismatch-Repair Deficiency Delineate Two Modes of Response to Anti-PD-1 Immunotherapy in Endometrial Carcinoma
- PMID: 36301137
- PMCID: PMC9905265
- DOI: 10.1158/2159-8290.CD-22-0686
Distinct Mechanisms of Mismatch-Repair Deficiency Delineate Two Modes of Response to Anti-PD-1 Immunotherapy in Endometrial Carcinoma
Abstract
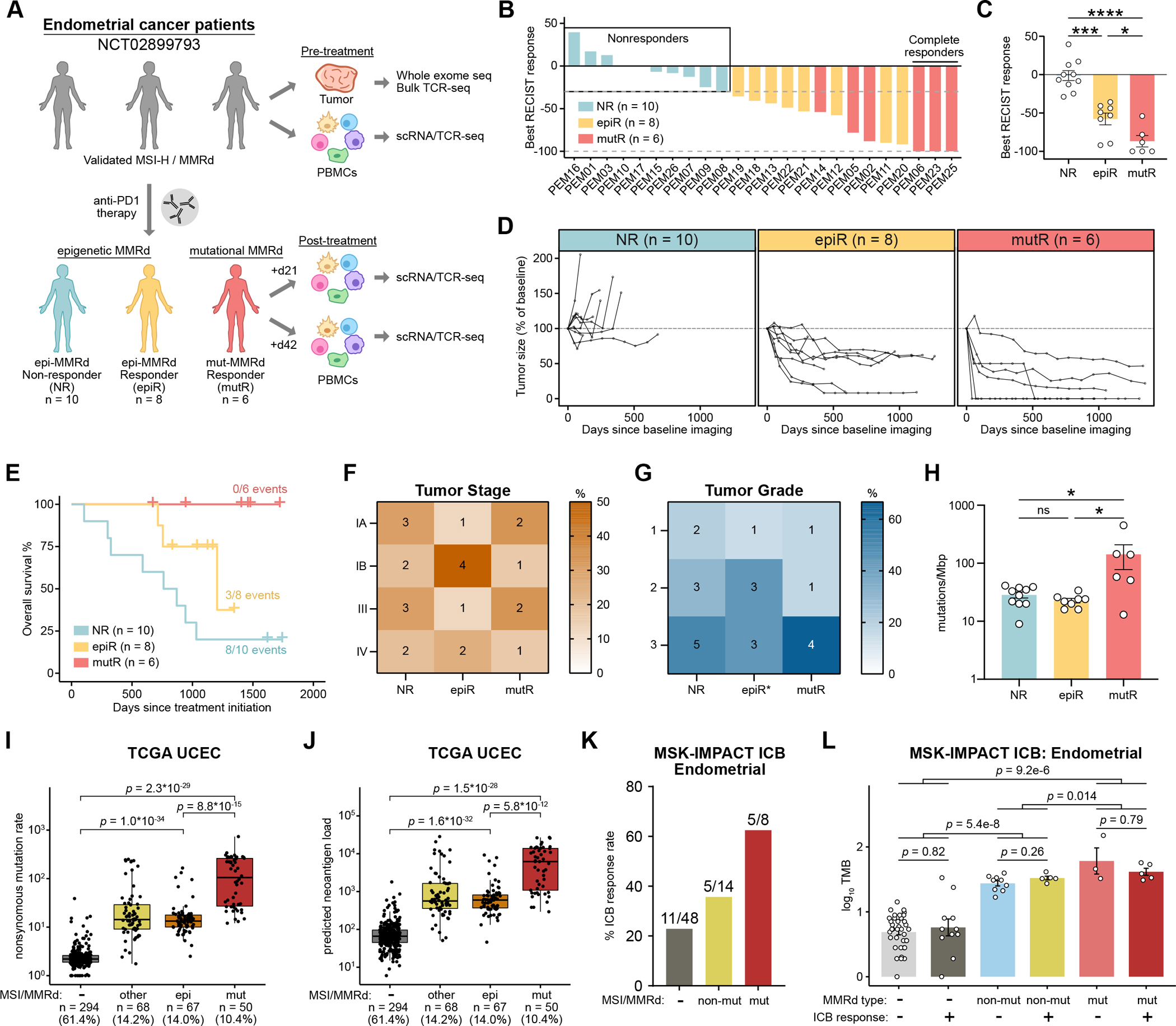
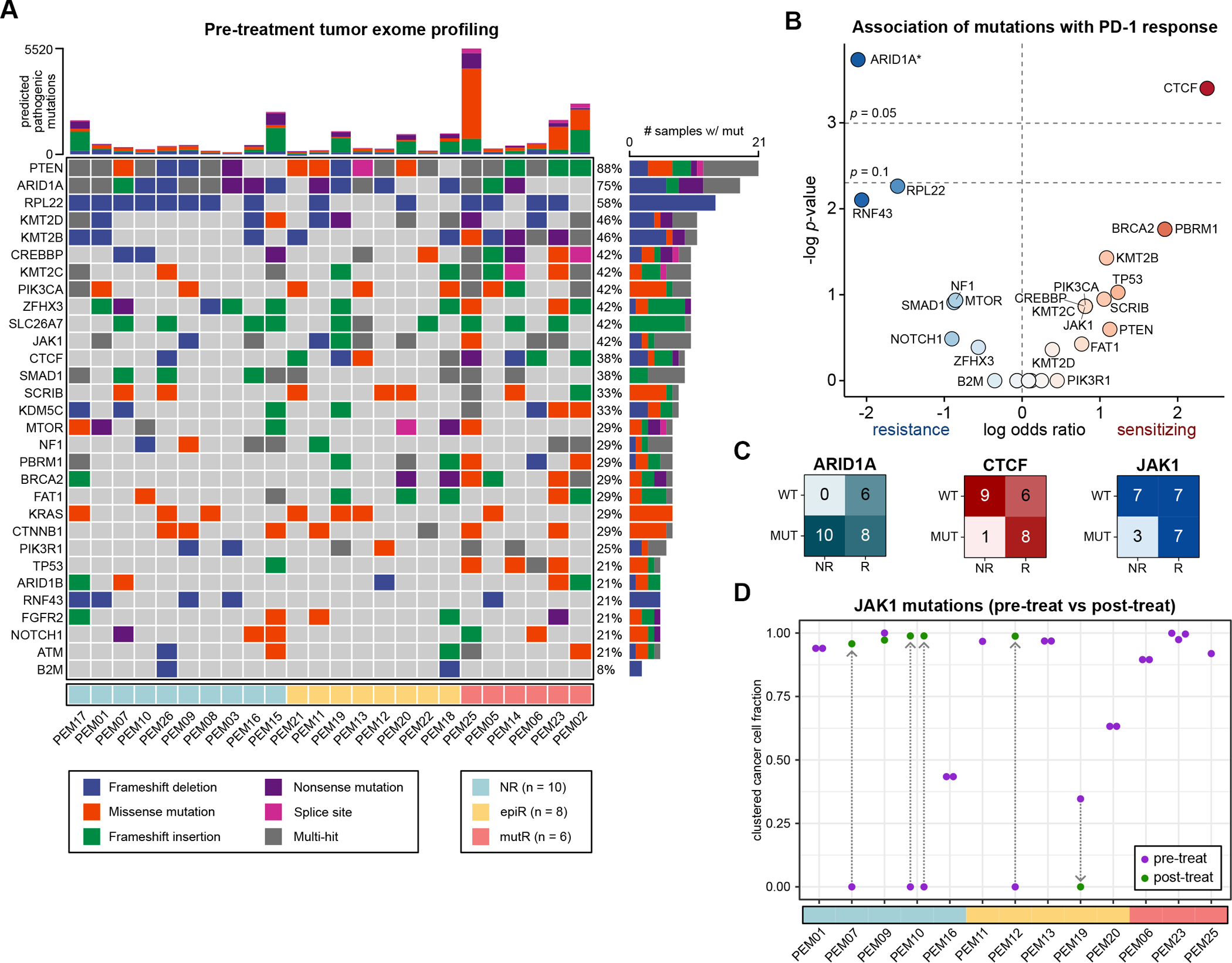
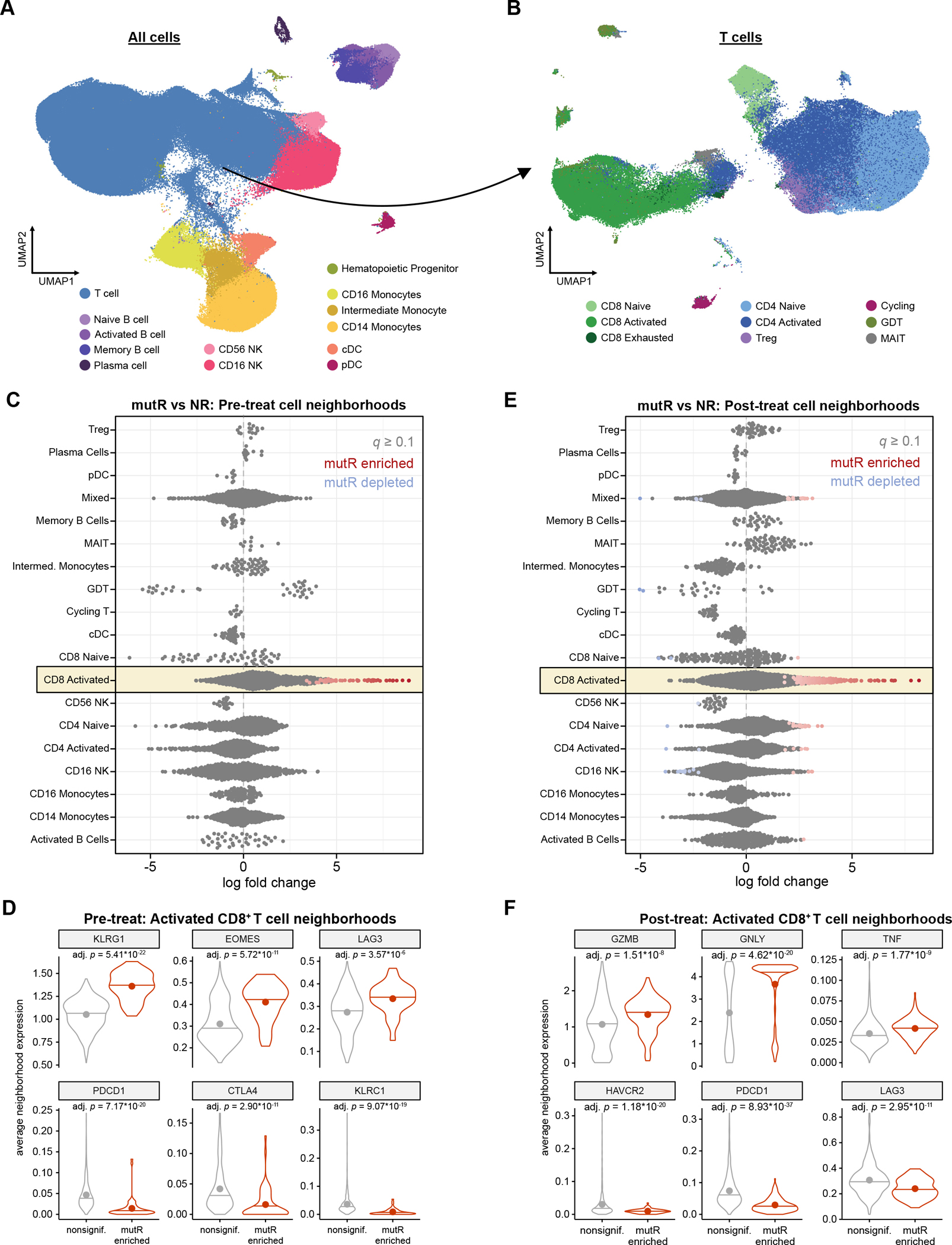
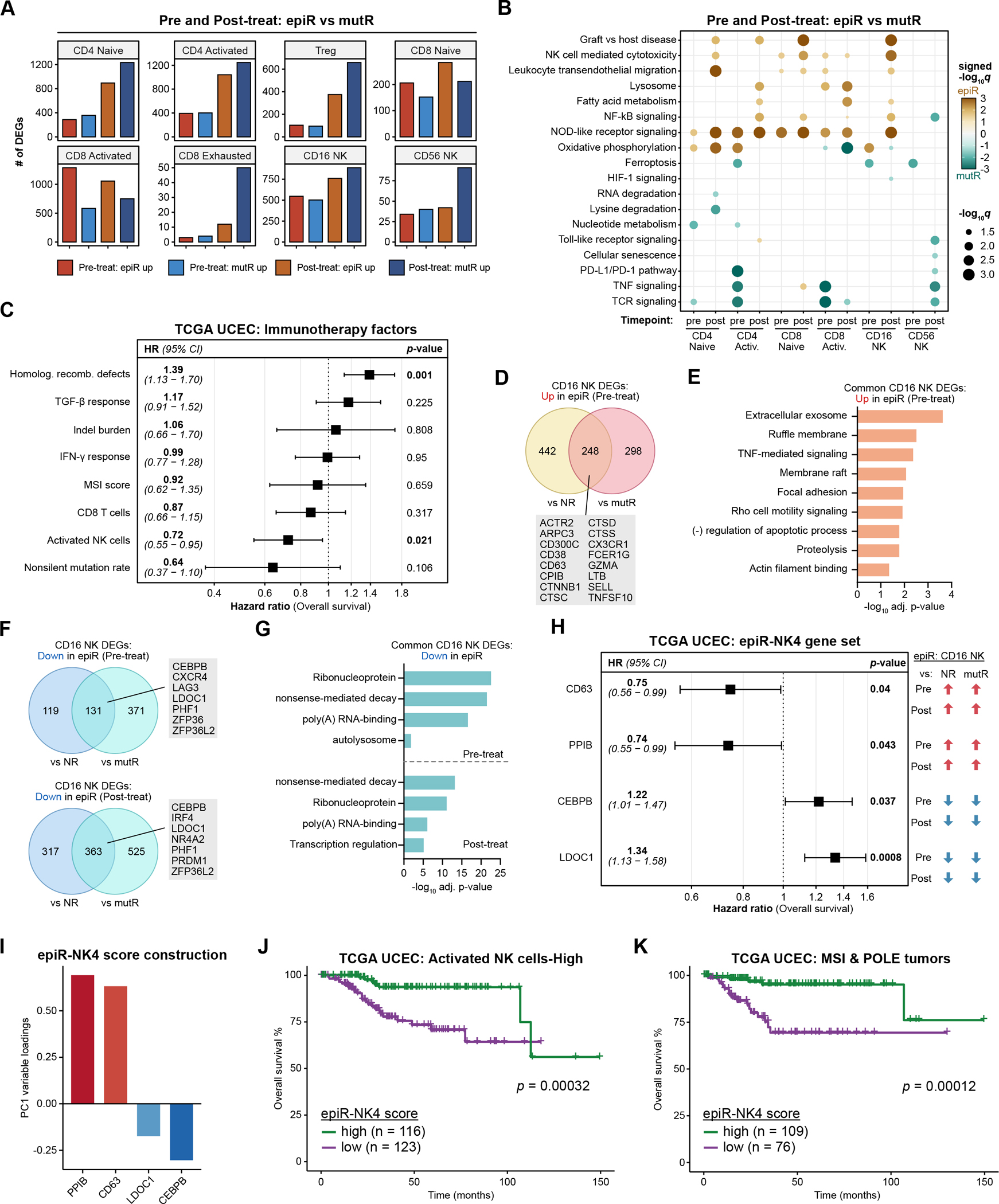
Mismatch repair-deficient (MMRd) cancers have varied responses to immune-checkpoint blockade (ICB). We conducted a phase II clinical trial of the PD-1 inhibitor pembrolizumab in 24 patients with MMRd endometrial cancer (NCT02899793). Patients with mutational MMRd tumors (6 patients) had higher response rates and longer survival than those with epigenetic MMRd tumors (18 patients). Mutation burden was higher in tumors with mutational MMRd compared with epigenetic MMRd; however, within each category of MMRd, mutation burden was not correlated with ICB response. Pretreatment JAK1 mutations were not associated with primary resistance to pembrolizumab. Longitudinal single-cell RNA-seq of circulating immune cells revealed contrasting modes of antitumor immunity for mutational versus epigenetic MMRd cancers. Whereas effector CD8+ T cells correlated with regression of mutational MMRd tumors, activated CD16+ NK cells were associated with ICB-responsive epigenetic MMRd tumors. These data highlight the interplay between tumor-intrinsic and tumor-extrinsic factors that influence ICB response.
Significance: The molecular mechanism of MMRd is associated with response to anti-PD-1 immunotherapy in endometrial carcinoma. Tumors with epigenetic MMRd or mutational MMRd are correlated with NK cell or CD8+ T cell-driven immunity, respectively. Classifying tumors by the mechanism of MMRd may inform clinical decision-making regarding cancer immunotherapy. This article is highlighted in the In This Issue feature, p. 247.
©2022 American Association for Cancer Research.
Conflict of interest statement
Conflict of Interest Statement:
Alessandro D. Santin reports grants or contracts from Immunomedics, Genentech, Puma, Gilead, Synthon, Boehringer-Ingelheim, Tesaro, and Eisai (to his institution) and consulting fees from Merck, Tesaro, and Eisai. The other authors declare no potential conflicts of interest.
Figures
References
-
- Hause RJ, Pritchard CC, Shendure J, Salipante SJ. Classification and characterization of microsatellite instability across 18 cancer types. Nat Med. 2016;22:1342–50. - PubMed
-
- Germano G, Lamba S, Rospo G, Barault L, Magrì A, Maione F, et al. Inactivation of DNA repair triggers neoantigen generation and impairs tumour growth. Nature. 2017;552:116–20. - PubMed
-
- André T, Shiu K-K, Kim TW, Jensen BV, Jensen LH, Punt C, et al. Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. New England Journal of Medicine. Massachusetts Medical Society; 2020;383:2207–18. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
