

Annual report to the nation on the status of cancer, part 1: National cancer statistics
- PMID: 36301149
- PMCID: PMC10092838
- DOI: 10.1002/cncr.34479
Annual report to the nation on the status of cancer, part 1: National cancer statistics
Abstract
Background: The American Cancer Society, the Centers for Disease Control and Prevention, the National Cancer Institute, and the North American Association of Central Cancer Registries collaborate to provide annual updates on cancer occurrence and trends in the United States.
Methods: Data on new cancer diagnoses during 2001-2018 were obtained from the North American Association of Central Cancer Registries' Cancer in North America Incidence file, which is comprised of data from Centers for Disease Control and Prevention-funded and National Cancer Institute-funded, population-based cancer registry programs. Data on cancer deaths during 2001-2019 were obtained from the National Center for Health Statistics' National Vital Statistics System. Five-year average incidence and death rates along with trends for all cancers combined and for the leading cancer types are reported by sex, racial/ethnic group, and age.
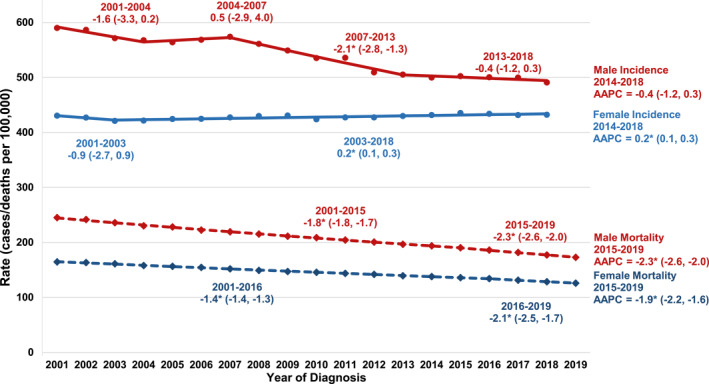
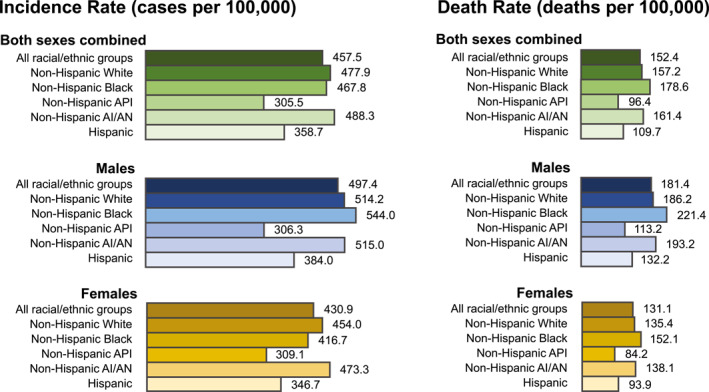
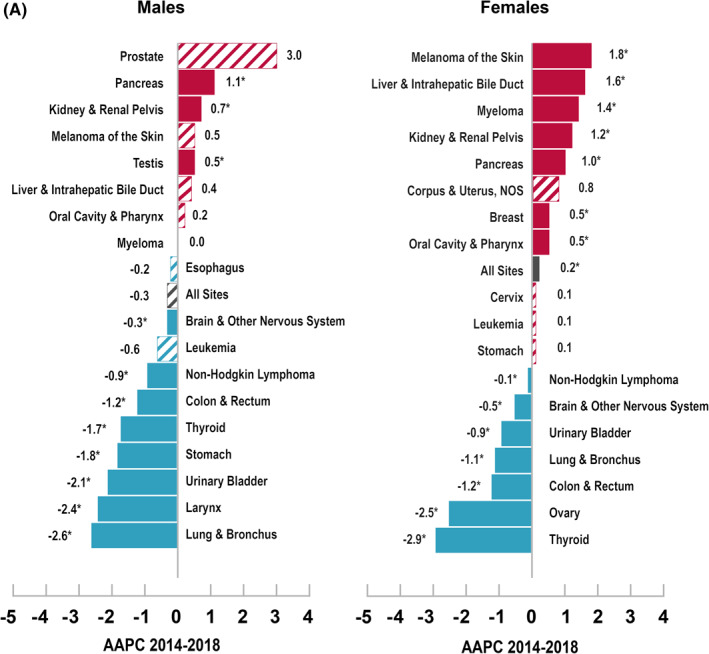
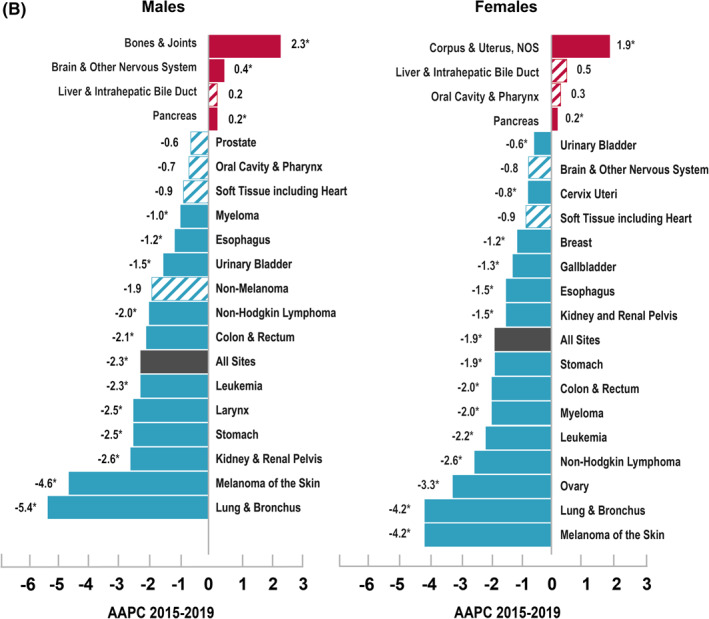
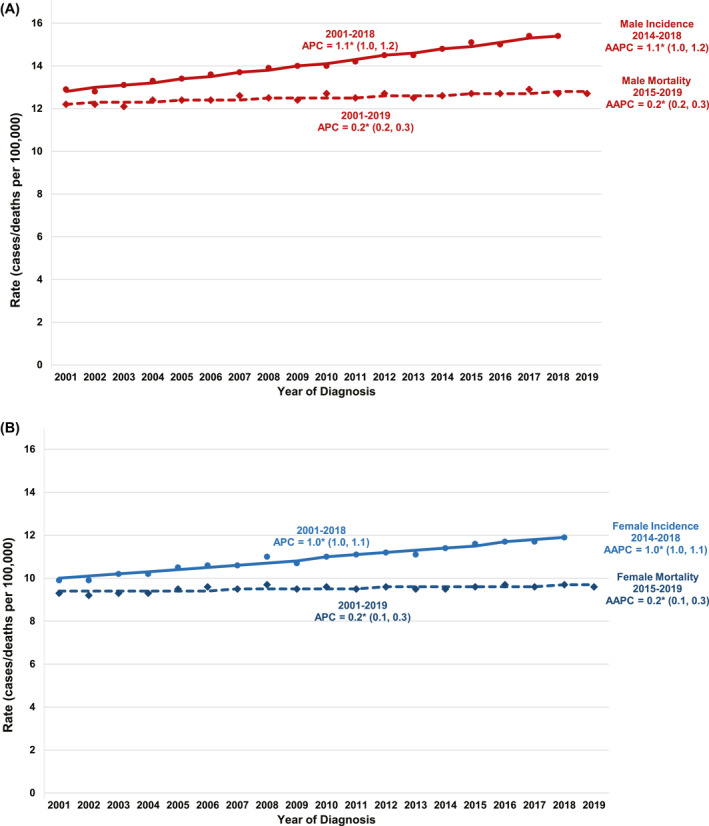
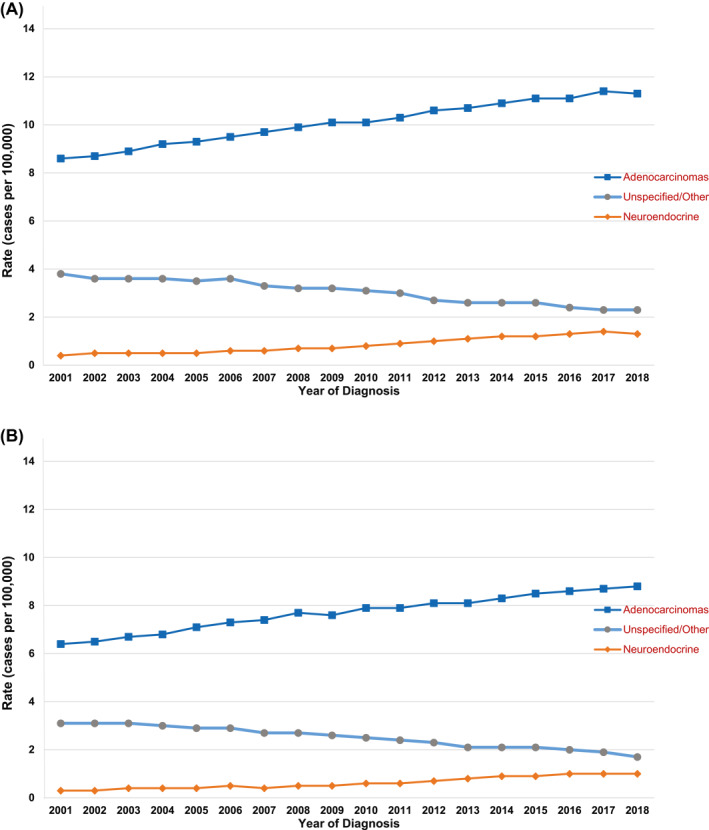
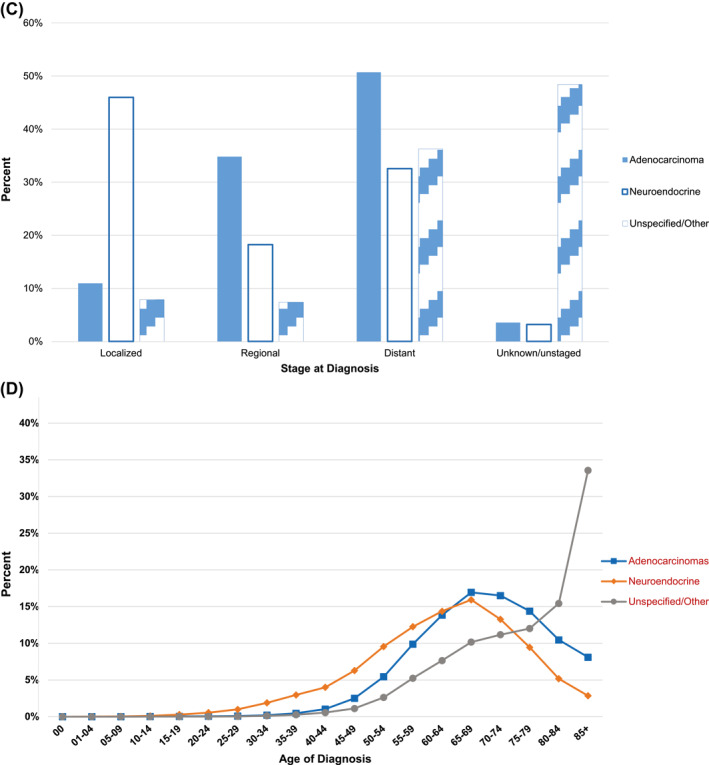
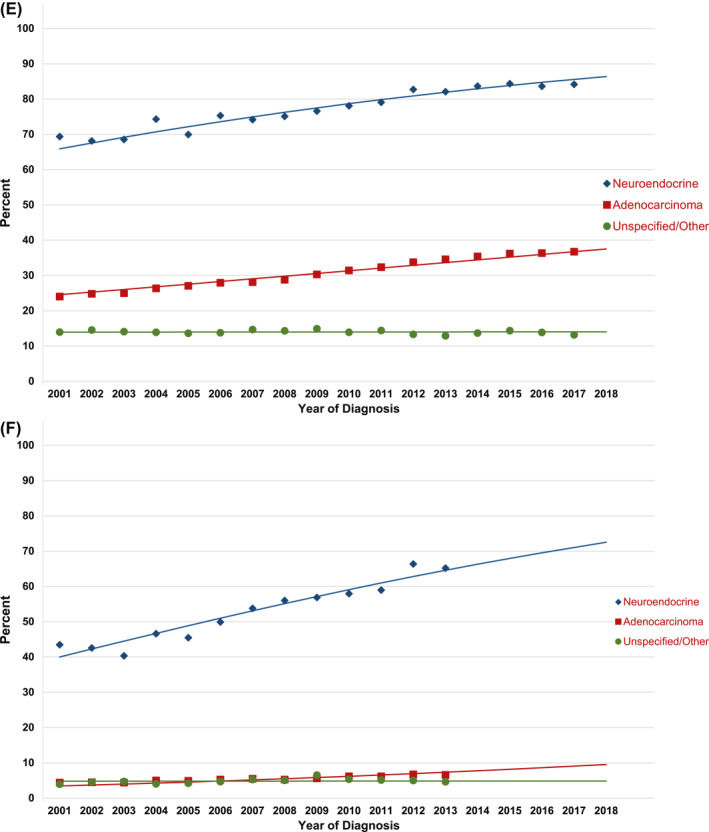
Results: Overall cancer incidence rates were 497 per 100,000 among males (ranging from 306 among Asian/Pacific Islander males to 544 among Black males) and 431 per 100,000 among females (ranging from 309 among Asian/Pacific Islander females to 473 among American Indian/Alaska Native females) during 2014-2018. The trend during the corresponding period was stable among males and increased 0.2% on average per year among females, with differing trends by sex, racial/ethnic group, and cancer type. Among males, incidence rates increased for three cancers (including pancreas and kidney), were stable for seven cancers (including prostate), and decreased for eight (including lung and larynx) of the 18 most common cancers considered in this analysis. Among females, incidence rates increased for seven cancers (including melanoma, liver, and breast), were stable for four cancers (including uterus), and decreased for seven (including thyroid and ovary) of the 18 most common cancers. Overall cancer death rates decreased by 2.3% per year among males and by 1.9% per year among females during 2015-2019, with the sex-specific declining trend reflected in every major racial/ethnic group. During 2015-2019, death rates decreased for 11 of the 19 most common cancers among males and for 14 of the 20 most common cancers among females, with the steepest declines (>4% per year) reported for lung cancer and melanoma. Five-year survival for adenocarcinoma and neuroendocrine pancreatic cancer improved between 2001 and 2018; however, overall incidence (2001-2018) and mortality (2001-2019) continued to increase for this site. Among children (younger than 15 years), recent trends were stable for incidence and decreased for mortality; and among, adolescents and young adults (aged 15-39 years), recent trends increased for incidence and declined for mortality.
Conclusions: Cancer death rates continued to decline overall, for children, and for adolescents and young adults, and treatment advances have led to accelerated declines in death rates for several sites, such as lung and melanoma. The increases in incidence rates for several common cancers in part reflect changes in risk factors, screening test use, and diagnostic practice. Racial/ethnic differences exist in cancer incidence and mortality, highlighting the need to understand and address inequities. Population-based incidence and mortality data inform prevention, early detection, and treatment efforts to help reduce the cancer burden in the United States.
Keywords: cancer; cancer death rate; incidence; mortality; pancreas.
© 2022 The Authors. Cancer published by Wiley Periodicals LLC on behalf of American Cancer Society. This article has been contributed to by US Government employees and their work is in the public domain in the USA.
Conflict of interest statement
Betsy A. Kohler reports personal fees from the National Firefighters Registry outside the submitted work and is a fiduciary officer of the North American Association of Central Cancer Registries. Charles Wiggins reports personal fees from the Northwest Portland Area Indian Health Board outside the submitted work and is a fiduciary officer of the International Association of Cancer Registries. William G. Cance reports personal fees from the University of North Carolina at Chapel Hill School of Medicine outside the submitted work, service on an ACRIN Data and Safety Monitoring Board, and has a spouse/partner who is a consultant for FAKnostics. The remaining authors made no disclosures.
Figures
References
-
- Sherman R, Firth R, Charlton M, et al., eds. Cancer in North America: 2014‐2018. Volume One: Combined Cancer Incidence for the United States, Canada and North America. North American Association of Central Cancer Registries, Inc.; 2021.
-
- Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin LH. International Classification of Diseases for Oncology. 3rd ed. World Health Organization; 2000. Accessed February 1, 2022. https://apps.who.int/iris/handle/10665/42344
-
- Swerdlow SH, Campo E, Harris NL, et al., eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Vol. 2. IARC Press; 2008.
-
- National Cancer Institute . Site Recode ICD‐O‐3/WHO 2008 Definition. SEER Data Reporting Tools. National Cancer Institute, Surveillance, Epidemiology, and End Results (SEER) Program. Accessed February 1, 2022. https://seer.cancer.gov/siterecode/icdo3_dwhoheme/
-
- World Health Organization. International Classification of Diseases for Oncology (ICD‐O) 3rd ed. 1st revision. World Health Organization; 2013. Accessed February 1, 2022. https://apps.who.int/iris/handle/10665/96612
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
