

A Comparison of the Effectiveness of Videolaryngoscopy and Macintosh Laryngoscopy in Intubation Attempts on Adult Patients
- PMID: 36301284
- PMCID: PMC9682947
- DOI: 10.5152/TJAR.2022.21367
A Comparison of the Effectiveness of Videolaryngoscopy and Macintosh Laryngoscopy in Intubation Attempts on Adult Patients
Abstract
Objective: This study aimed to compare the effectiveness of videolaryngoscopy and Macintosh laryngoscopy on adult patients who were scheduled for elective surgery under general anaesthesia.
Methods: Of the 200 adult patients who were scheduled to undergo general anaesthesia, 100 were intubated with a videolaryngoscope and 100 with a Macintosh laryngoscope. The patients' age, sex, American Society of Anesthesiologists score, height, weight, body mass index, smoking and alcohol habits, comorbidity, and neck circumference were recorded. Their El-Ganzouri Risk Index score, which considers the parameters of mouth opening, thyromental distance, Mallampati score, neck movement, propensity for prognathism, body weight, and history of difficult intubation, was also calculated and recorded. The time to achieve intubation was then recorded. The number of intubation attempts, number of cases of difficult intubation, Cormack-Lehane scores, and incidences of trauma or complication were also evaluated.
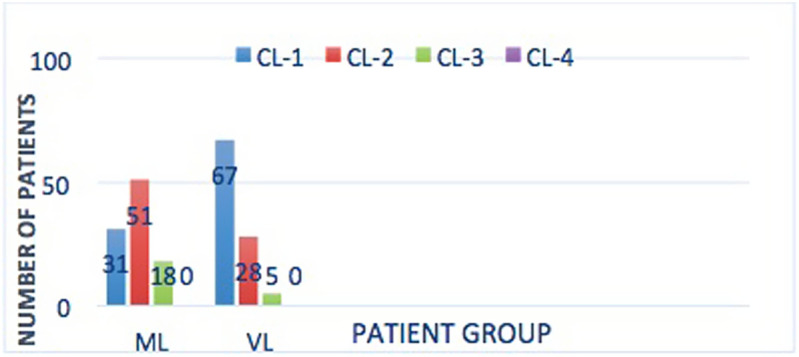
Results: The mean intubation time was found to be significantly lower in the videolaryngoscope group compared to the Macintosh laryngoscope group. Although the number of patients with difficult intubation was high in the videolaryngoscope group, when we evaluated their glottic view, the Cormack-Lehane score was found to be significantly lower. The number and ratio of complications due to intubation were lower in the videolaryngoscope group compared to the Macintosh laryngoscopy group.
Conclusions: In patients undergoing endotracheal intubation for general anaesthesia, it was concluded that videolaryngoscopy is superior to Macintosh laryngoscopy as it enlarges the glottic view, shortens the time to achieve intubation, facilitates intubation, and has less risk of complications.
Figures

References
-
- Hagberg CA, Artime CA. Airway management in the adult. In: Miller RD.ed. Miller’s Anesthesia. 8th ed. Philadelphia; Elsevier, Saunder; 2015:1647 16 84.
LinkOut - more resources
Full Text Sources