

Early administration of remdesivir may reduce mortality in hospitalized COVID-19 patients : A propensity score matched analysis
- PMID: 36301355
- PMCID: PMC9610353
- DOI: 10.1007/s00508-022-02098-9
Early administration of remdesivir may reduce mortality in hospitalized COVID-19 patients : A propensity score matched analysis
Abstract
Background: Remdesivir is the only antiviral agent approved for the treatment of hospitalized coronavirus disease 2019 (COVID-19) patients requiring supplemental oxygen. Studies show conflicting results regarding its effect on mortality.
Methods: In this single center observational study, we included adult hospitalized COVID-19 patients. Patients who were treated with remdesivir were compared to controls. Remdesivir was administered for 5 days. To adjust for any imbalances in our cohort, a propensity score matched analysis was performed. The aim of our study was to analyze the effect of remdesivir on in-hospital mortality and length of stay (LOS).
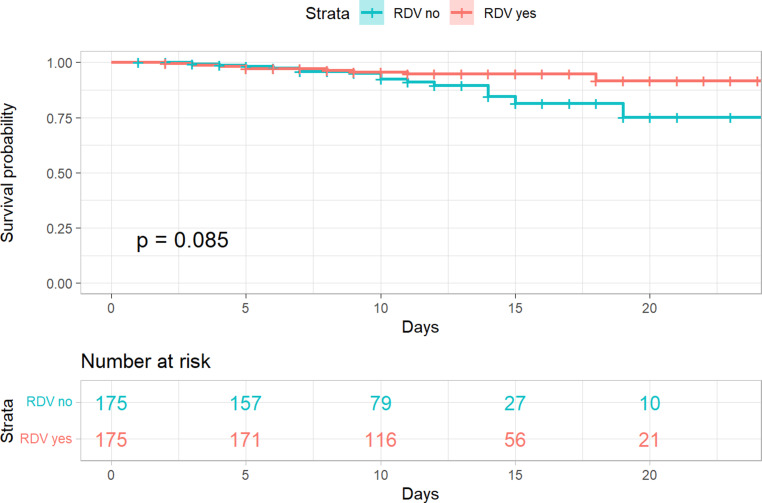
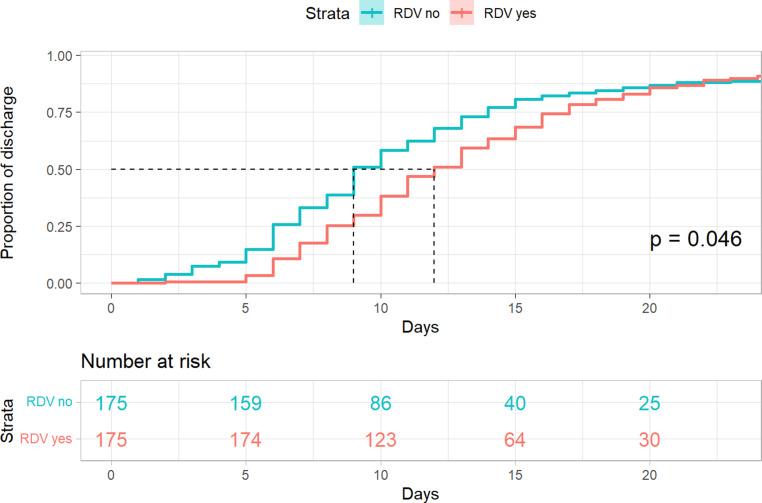
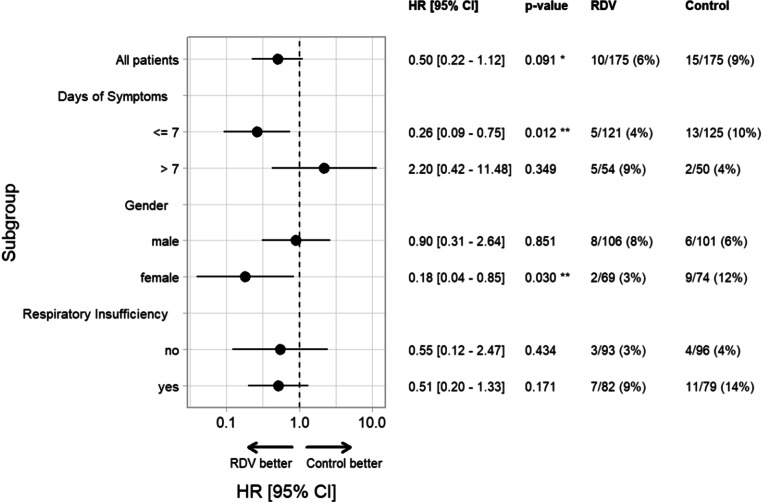
Results: After propensity score matching, 350 patients (175 remdesivir, 175 controls) were included in our analysis. Overall, in-hospital mortality was not significantly different between groups remdesivir 5.7% [10/175] vs. control 8.6% [15/175], hazard ratio 0.50, 95% confidence interval (CI) 0.22-1.12, p = 0.091. Subgroup analysis showed a significant reduction of in-hospital mortality in patients who were treated with remdesivir ≤ 7 days of symptom onset remdesivir 4.2% [5/121] vs. control 10.4% [13/125], hazard ratio 0.26, 95% CI 0.09 to 0.75, p = 0.012 and in female patients remdesivir 2.9% [2/69] vs. control 12.2% [9/74], hazard ratio 0.18 95%CI 0.04 to 0.85, p = 0.03. Patients in the remdesivir group had a significantly longer LOS (11 days vs. 9 days, p = 0.046).
Conclusion: Remdesivir did not reduce in-hospital mortality in our whole propensity score matched cohort, but subgroup analysis showed a significant mortality reduction in female patients and in patients treated within ≤ 7 days of symptom onset. Remdesivir may reduce mortality in patients who are treated in the early stages of illness.
Keywords: Austria; Gender differences; In-hospital mortality; Length of stay; Within 7 days.
© 2022. The Author(s), under exclusive licence to Springer-Verlag GmbH Austria, part of Springer Nature.
Conflict of interest statement
M. Karolyi, L. Kaltenegger, E. Pawelka, A. Kuran, M. Platzer, D. Totschnig, F. Koenig, W. Hoepler, H. Laferl, S. Omid, T. Seitz, M. Traugott, S. Arthofer, L. Erlbeck, S. Jaeger, A. Kettenbach, A. Assinger, C. Wenisch and A. Zoufaly declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
