

Association of Immune-Related Adverse Event Management With Survival in Patients With Advanced Melanoma
- PMID: 36301521
- PMCID: PMC9614679
- DOI: 10.1001/jamaoncol.2022.5041
Association of Immune-Related Adverse Event Management With Survival in Patients With Advanced Melanoma
Abstract
Importance: Management of checkpoint inhibitor-induced immune-related adverse events (irAEs) is primarily based on expert opinion. Recent studies have suggested detrimental effects of anti-tumor necrosis factor on checkpoint-inhibitor efficacy.
Objective: To determine the association of toxic effect management with progression-free survival (PFS), overall survival (OS), and melanoma-specific survival (MSS) in patients with advanced melanoma treated with first-line ipilimumab-nivolumab combination therapy.
Design, setting, and participants: This population-based, multicenter cohort study included patients with advanced melanoma experiencing grade 3 and higher irAEs after treatment with first-line ipilimumab and nivolumab between 2015 and 2021. Data were collected from the Dutch Melanoma Treatment Registry. Median follow-up was 23.6 months.
Main outcomes and measures: The PFS, OS, and MSS were analyzed according to toxic effect management regimen. Cox proportional hazard regression was used to assess factors associated with PFS and OS.
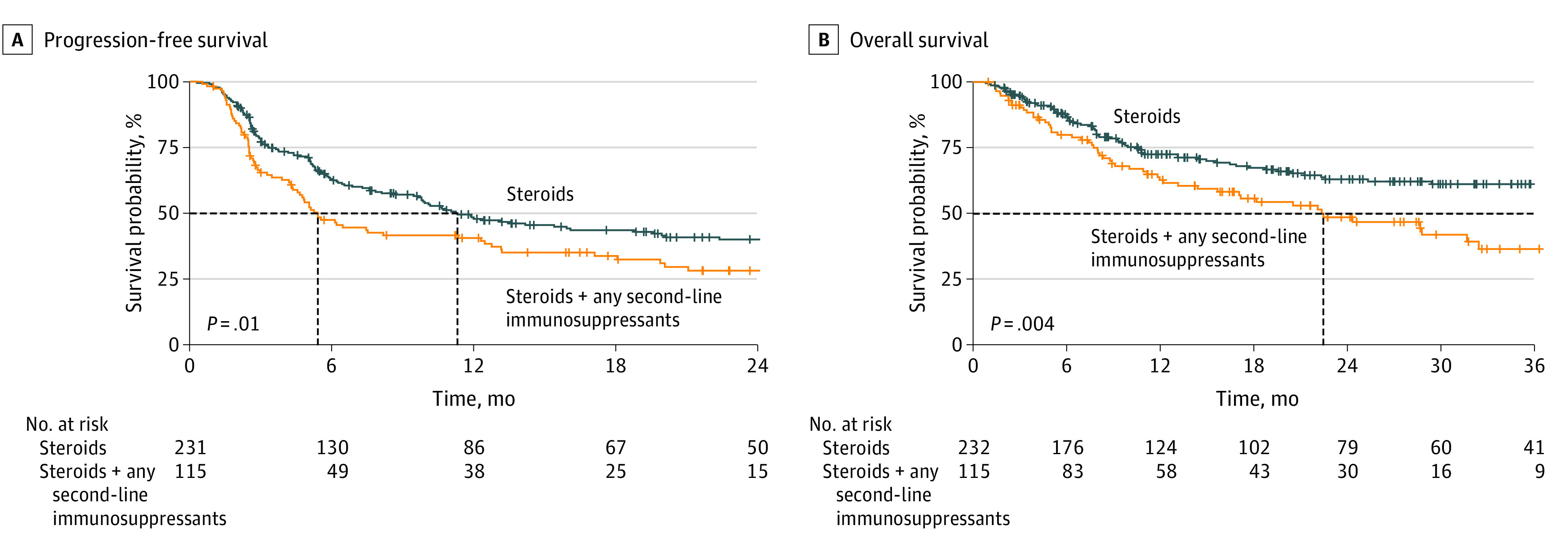
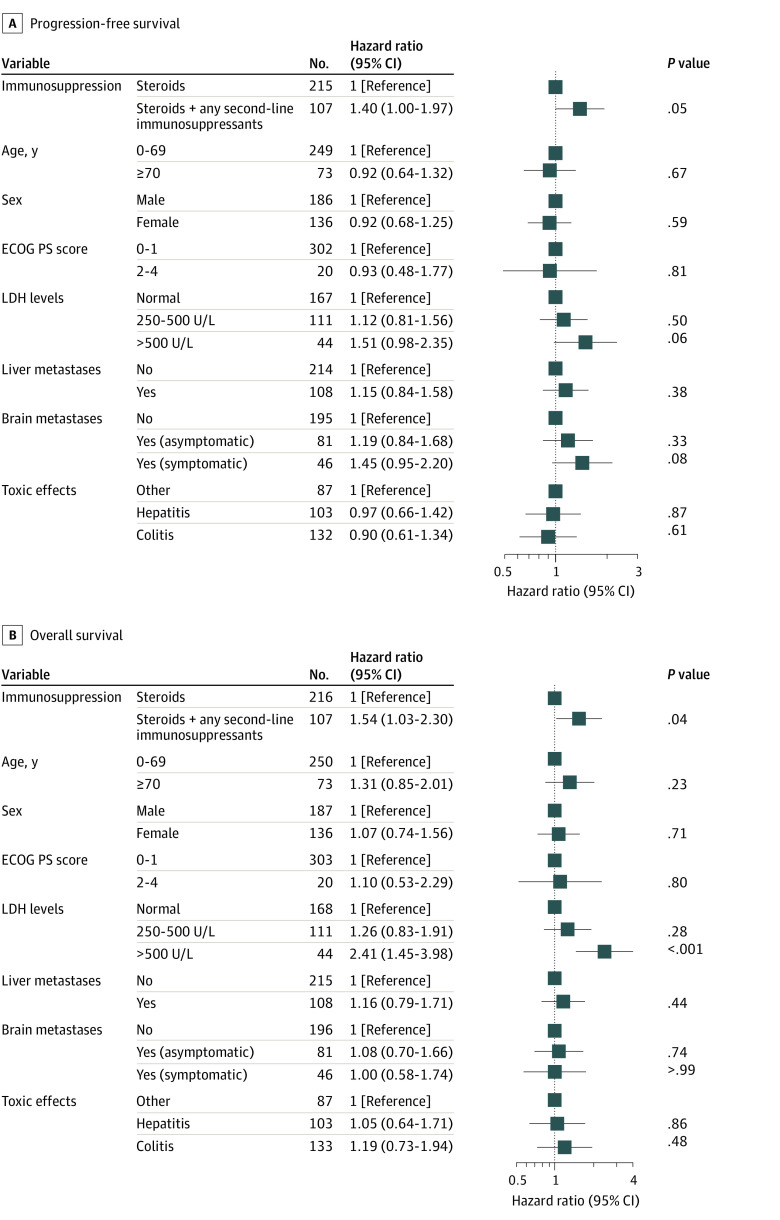
Results: Of 771 patients treated with ipilimumab and nivolumab, 350 patients (median [IQR] age, 60.0 [51.0-68.0] years; 206 [58.9%] male) were treated with immunosuppression for severe irAEs. Of these patients, 235 received steroids alone, and 115 received steroids with second-line immunosuppressants. Colitis and hepatitis were the most frequently reported types of toxic effects. Except for type of toxic effect, no statistically significant differences existed at baseline. Median PFS was statistically significantly longer for patients treated with steroids alone compared with patients treated with steroids plus second-line immunosuppressants (11.3 [95% CI, 9.6-19.6] months vs 5.4 [95% CI, 4.5-12.4] months; P = .01). Median OS was also statistically significantly longer for the group receiving steroids alone compared with those receiving steroids plus second-line immunosuppressants (46.1 months [95% CI, 39.0 months-not reached (NR)] vs 22.5 months [95% CI, 36.5 months-NR]; P = .04). Median MSS was also better in the group receiving steroids alone compared with the group receiving steroids plus second-line immunosuppressants (NR [95% CI, 46.1 months-NR] vs 28.8 months [95% CI, 20.5 months-NR]; P = .006). After adjustment for potential confounders, patients treated with steroids plus second-line immunosuppressants showed a trend toward a higher risk of progression (adjusted hazard ratio, 1.40 [95% CI, 1.00-1.97]; P = .05) and had a higher risk of death (adjusted hazard ratio, 1.54 [95% CI, 1.03-2.30]; P = .04) compared with those receiving steroids alone.
Conclusions and relevance: In this cohort study, second-line immunosuppression for irAEs was associated with impaired PFS, OS, and MSS in patients with advanced melanoma treated with first-line ipilimumab and nivolumab. These findings stress the importance of assessing the effects of differential irAE management strategies, not only in patients with melanoma but also other tumor types.
Conflict of interest statement
Figures
Comment in
-
Steroid Dose and Duration, Immortal Time Bias, and Survival After High-grade Immune-Related Adverse Events.JAMA Oncol. 2023 May 1;9(5):723-724. doi: 10.1001/jamaoncol.2023.0100. JAMA Oncol. 2023. PMID: 36892846 No abstract available.
References
-
- Horvat TZ, Adel NG, Dang TO, et al. . Immune-related adverse events, need for systemic immunosuppression, and effects on survival and time to treatment failure in patients with melanoma treated with ipilimumab at Memorial Sloan Kettering Cancer Center. J Clin Oncol. 2015;33(28):3193-3198. doi:10.1200/JCO.2015.60.8448 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
