

Polypharmacy and multiple sclerosis: A population-based study
- PMID: 36301629
- PMCID: PMC9896267
- DOI: 10.1177/13524585221122207
Polypharmacy and multiple sclerosis: A population-based study
Abstract
Background: Little is known about polypharmacy and multiple sclerosis (MS).
Objectives: To estimate polypharmacy prevalence in a population-based MS cohort and compare persons with/without polypharmacy.
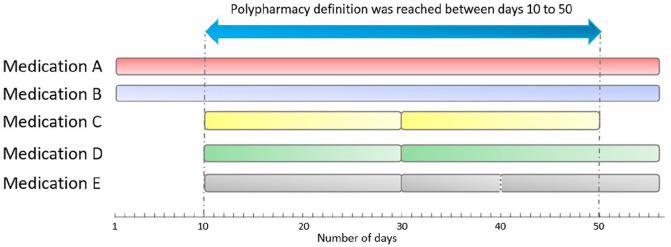
Methods: Using administrative and pharmacy data from Canada, we estimated polypharmacy prevalence (⩾5 concurrent medications for >30 consecutive days) in MS individuals in 2017. We compared the characteristics of persons with/without polypharmacy and described the number of polypharmacy days, the most common medication classes contributing to polypharmacy and hyper-polypharmacy prevalence (⩾10 medications).
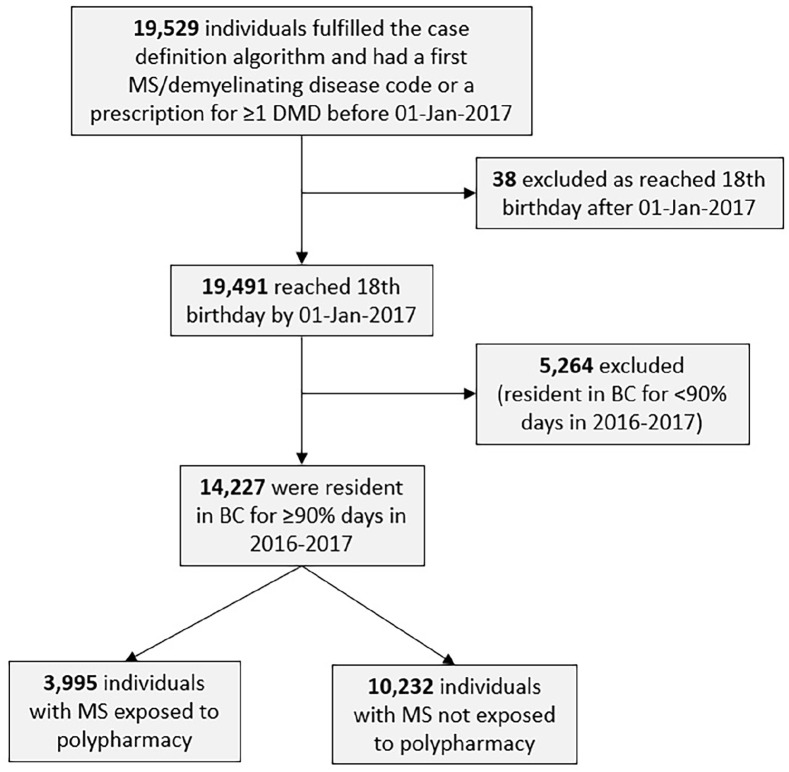
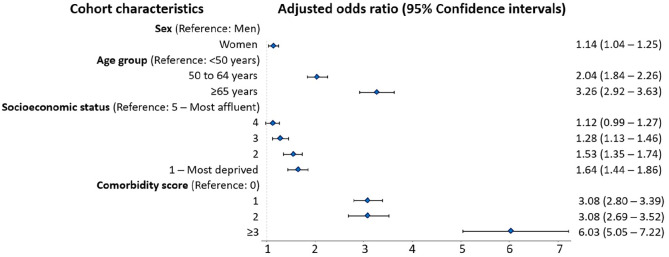
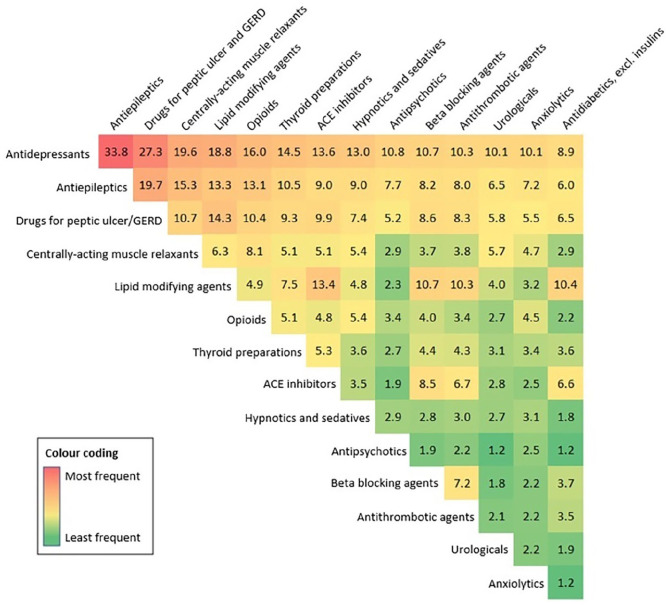
Results: Of 14,227 included individuals (75% women), mean age = 55.4 (standard deviation (SD): 13.2) years; 28% (n = 3995) met criteria for polypharmacy (median polypharmacy days = 273 (interquartile range (IQR): 120-345)). Odds of polypharmacy were higher for women (adjusted odds ratio (aOR) = 1.14; 95% confidence intervals (CI):1.04-1.25), older individuals (aORs 50-64 years = 2.04; 95% CI:1.84-2.26; ⩾65 years = 3.26; 95% CI: 2.92-3.63 vs. <50 years), those with more comorbidities (e.g. ⩾3 vs. none, aOR = 6.03; 95% CI: 5.05-7.22) and lower socioeconomic status (SES) (e.g. most (SES-Q1) vs. least deprived (SES-Q5) aOR = 1.64; 95% CI: 1.44-1.86). Medication classes most commonly contributing to polypharmacy were as follows: antidepressants (66% of polypharmacy days), antiepileptics (47%), and peptic ulcer drugs (41%). Antidepressants were most frequently co-prescribed with antiepileptics (34% of polypharmacy days) and peptic ulcer drugs (27%). Five percent of persons (716/14,227) experienced hyper-polypharmacy.
Conclusion: More than one in four MS persons met criteria for polypharmacy. The odds of polypharmacy were higher for women, older persons, and those with more comorbidities, but lower SES.
Keywords: MS; pharmacoepidemiology; polypharmacy; population-based data; prescription medication use.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.C. receives funding from the MS Society of Canada’s endMS Postdoctoral Fellowship and the Michael Smith Foundation for Health Research Trainee Award. H.S.N. has received funding from the Multiple Sclerosis Society of Canada’s endMS Postdoctoral Fellowship, and the Michael Smith Foundation for Health Research Trainee Award. F.Z. and Y.Z. have no disclosures. H.T. has, in the last 5 years, received research support from the Canada Research Chair Program, the National Multiple Sclerosis Society, the Canadian Institutes of Health Research, the Multiple Sclerosis Society of Canada, and the Multiple Sclerosis Scientific Research Foundation. In addition, in the last 5 years, has had travel expenses or registration fees prepaid or reimbursed to present at CME conferences from the Consortium of MS Centers (2018), National MS Society (2016, 2018), ECTRIMS/ACTRIMS (2015, 2016, 2017, 2018, 2019, 2020, 2021, and 2022), American Academy of Neurology (2015, 2016, and 2019). Speaker honoraria are either declined or donated to an MS charity or to an unrestricted grant for use by HT’s research group.
Figures
Comment in
-
Polypharmacy in multiple sclerosis: More is not necessarily better.Mult Scler. 2023 Jan;29(1):3-5. doi: 10.1177/13524585221129964. Epub 2022 Oct 14. Mult Scler. 2023. PMID: 36239156 No abstract available.
Similar articles
-
Antidepressant Use Among People Prescribed Opioids for Chronic Noncancer Pain.Pain Med. 2019 Dec 1;20(12):2450-2458. doi: 10.1093/pm/pnz009. Pain Med. 2019. PMID: 30861530 Free PMC article.
-
Trends in central nervous system-active polypharmacy among people with multiple sclerosis.Mult Scler. 2024 Aug;30(9):1139-1150. doi: 10.1177/13524585241251986. Epub 2024 May 15. Mult Scler. 2024. PMID: 38751229 Free PMC article.
-
Prevalence of Central Nervous System-Active Polypharmacy Among Older Adults With Dementia in the US.JAMA. 2021 Mar 9;325(10):952-961. doi: 10.1001/jama.2021.1195. JAMA. 2021. PMID: 33687462 Free PMC article.
-
Factors associated with polypharmacy and the prescription of multiple medications among persons living with HIV (PLWH) compared to non-PLWH.AIDS Care. 2015;27(12):1443-8. doi: 10.1080/09540121.2015.1109583. Epub 2015 Nov 26. AIDS Care. 2015. PMID: 26608408
-
Prescribing of disease modifying agents in older adults with multiple sclerosis.Mult Scler Relat Disord. 2022 Jan;57:103308. doi: 10.1016/j.msard.2021.103308. Epub 2021 Oct 5. Mult Scler Relat Disord. 2022. PMID: 35158421
Cited by
-
Personality traits in patients with multiple sclerosis: their association with nicotine dependence and polypharmacy.Ther Adv Neurol Disord. 2024 Oct 14;17:17562864241279118. doi: 10.1177/17562864241279118. eCollection 2024. Ther Adv Neurol Disord. 2024. PMID: 39411724 Free PMC article.
-
Comment on "Cerebrospinal fluid camk2a levels at baseline predict long-term progression in multiple sclerosis. Clinical Proteomics".Clin Proteomics. 2023 Oct 25;20(1):46. doi: 10.1186/s12014-023-09433-w. Clin Proteomics. 2023. PMID: 37880604 Free PMC article. No abstract available.
-
Should we stay or should we go? Recent insights on drug discontinuation in multiple sclerosis.Neurol Res Pract. 2025 Apr 21;7(1):25. doi: 10.1186/s42466-025-00379-y. Neurol Res Pract. 2025. PMID: 40254626 Free PMC article. Review.
-
Antibiotic Utilization Among People With Multiple Sclerosis in the Netherlands, 2018-2020.Pharmacoepidemiol Drug Saf. 2024 Dec;33(12):e70070. doi: 10.1002/pds.70070. Pharmacoepidemiol Drug Saf. 2024. PMID: 39662986 Free PMC article.
-
Integrating Clinical Pharmacy Services Into Comprehensive Multiple Sclerosis Care Teams: A Narrative Review of 4 Models.Int J MS Care. 2025 Apr 21;27(Q2):117-124. doi: 10.7224/1537-2073.2024-019. eCollection 2025 Apr. Int J MS Care. 2025. PMID: 40275992 Free PMC article. Review.
References
-
- Halli-Tierney A, Scarbrough C, Carroll D. Polypharmacy: Evaluating risks and deprescribing. Am Fam Physician 2019; 100(1): 32–38. - PubMed
-
- World Health Organization. Medication safety in polypharmacy: Technical report. World Health Organization, 2019, https://apps.who.int/iris/handle/10665/325454
-
- Hales CM, Servais J, Martin CB, et al.. Prescription drug use among adults aged 40-79 in the United States and Canada. NCHS Data Brief 2019; 347: 1–8. - PubMed
-
- Toosy A, Ciccarelli O, Thompson A. Symptomatic treatment and management of multiple sclerosis. Handb Clin Neurol 2014; 122: 513–562. - PubMed
-
- Marrie RA. Comorbidity in multiple sclerosis: Implications for patient care. Nat Rev Neurol 2017; 13(6): 375–382. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
