

Ascent rate and the Lake Louise scoring system: An analysis of one year of emergency ward entries for high-altitude sickness at the Mustang district hospital, Nepal
- PMID: 36301827
- PMCID: PMC9612449
- DOI: 10.1371/journal.pone.0276901
Ascent rate and the Lake Louise scoring system: An analysis of one year of emergency ward entries for high-altitude sickness at the Mustang district hospital, Nepal
Abstract
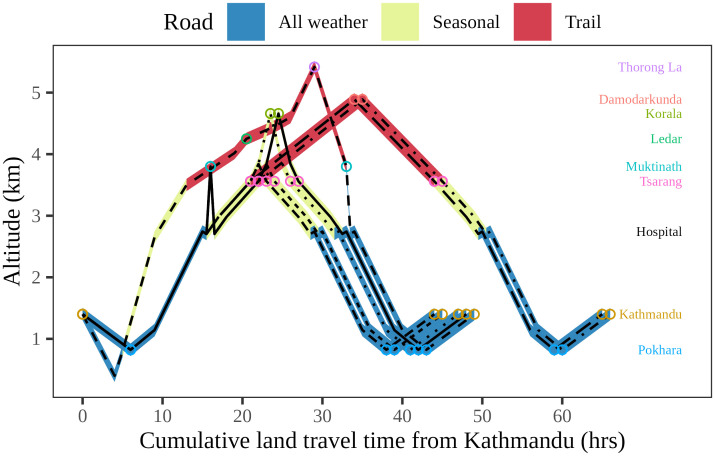
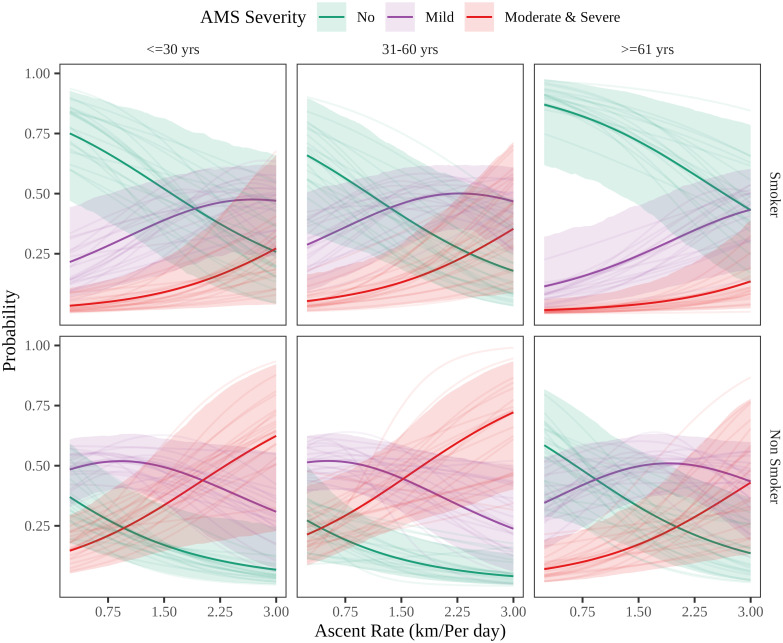
More travellers are making swift ascents to higher altitudes without sufficient acclimatization or pharmaceutical prophylaxis as road connectivity develops in the Himalayan region of Nepal. Our study connects ascent rate with prevalence and severity of acute mountain sickness (AMS) among patients admitted to the emergency ward of the Mustang district hospital in Nepal. A register-based, cross-sectional study was conducted between June 2018 and June 2019 to explore associations of Lake Louise scores with ascent profile, sociodemographic characteristics, and comorbidities using chi-square test, t-test, and Bayesian logistic regression. Of 105 patients, incidence of AMS was 74%, of which 61%, 36%, and 3% were mild, moderate, and severe cases, respectively. In the Bayesian-ordered logistic model of AMS severity, ascent rate (odds ratio 3.13) and smoking (odds ratio 0.16) were significant at a 99% credible interval. Based on the model-derived counterfactual, the risk of developing moderate or severe AMS for a middle-aged, non-smoking male traveling from Pokhara to Muktinath (2978m altitude gain) in a single day is twice that of making the ascent in three days. Ascent rate was strongly associated with the likelihood of developing severe AMS among travellers with AMS symptoms visiting Mustang Hospital's Emergency Ward.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Dynamics in the prevalence and clinical manifestations of acute mountain sickness of different ascent protocols during high altitudes exposure.Front Public Health. 2024 Nov 21;12:1472935. doi: 10.3389/fpubh.2024.1472935. eCollection 2024. Front Public Health. 2024. PMID: 39639900 Free PMC article.
-
Changes in metabolic and hematologic laboratory values with ascent to altitude and the development of acute mountain sickness in Nepalese pilgrims.Wilderness Environ Med. 2006 Fall;17(3):171-7. doi: 10.1580/pr43-04. Wilderness Environ Med. 2006. PMID: 17078312
-
Hypertension and Acute Mountain Sickness in Himalayan Trekkers in Nepal: An Observational Cohort Study.Wilderness Environ Med. 2020 Jun;31(2):157-164. doi: 10.1016/j.wem.2020.01.004. Epub 2020 Mar 21. Wilderness Environ Med. 2020. PMID: 32205041 Free PMC article.
-
The 2018 Lake Louise Acute Mountain Sickness Score.High Alt Med Biol. 2018 Mar;19(1):4-6. doi: 10.1089/ham.2017.0164. Epub 2018 Mar 13. High Alt Med Biol. 2018. PMID: 29583031 Free PMC article.
-
Sex-based differences in the prevalence of acute mountain sickness: a meta-analysis.Mil Med Res. 2019 Dec 9;6(1):38. doi: 10.1186/s40779-019-0228-3. Mil Med Res. 2019. PMID: 31813379 Free PMC article. Review.
Cited by
-
Risk factors associated with high altitude sickness among travelers: A case control study in Himalaya district of Nepal.PLOS Glob Public Health. 2025 Feb 7;5(2):e0004241. doi: 10.1371/journal.pgph.0004241. eCollection 2025. PLOS Glob Public Health. 2025. PMID: 39919099 Free PMC article.
-
Sleep loss effects on physiological and cognitive responses to systemic environmental hypoxia.Front Physiol. 2022 Dec 12;13:1046166. doi: 10.3389/fphys.2022.1046166. eCollection 2022. Front Physiol. 2022. PMID: 36579023 Free PMC article. Review.
-
Dynamics in the prevalence and clinical manifestations of acute mountain sickness of different ascent protocols during high altitudes exposure.Front Public Health. 2024 Nov 21;12:1472935. doi: 10.3389/fpubh.2024.1472935. eCollection 2024. Front Public Health. 2024. PMID: 39639900 Free PMC article.
References
-
- Hackett P. High-altitude medicine. Wilderness medicine. 2001:2–43.
MeSH terms
LinkOut - more resources
Full Text Sources
