

Gallbladder cancer
- PMID: 36302789
- PMCID: PMC12314663
- DOI: 10.1038/s41572-022-00398-y
Gallbladder cancer
Erratum in
-
Publisher Correction: Gallbladder cancer.Nat Rev Dis Primers. 2022 Nov 18;8(1):75. doi: 10.1038/s41572-022-00408-z. Nat Rev Dis Primers. 2022. PMID: 36400795 No abstract available.
Abstract
Gallbladder cancer (GBC) is the most common cancer of the biliary tract, characterized by a very poor prognosis when diagnosed at advanced stages owing to its aggressive behaviour and limited therapeutic options. Early detection at a curable stage remains challenging because patients rarely exhibit symptoms; indeed, most GBCs are discovered incidentally following cholecystectomy for symptomatic gallbladder stones. Long-standing chronic inflammation is an important driver of GBC, regardless of the lithiasic or non-lithiasic origin. Advances in omics technologies have provided a deeper understanding of GBC pathogenesis, uncovering mechanisms associated with inflammation-driven tumour initiation and progression. Surgical resection is the only treatment with curative intent for GBC but very few cases are suitable for resection and most adjuvant therapy has a very low response rate. Several unmet clinical needs require to be addressed to improve GBC management, including discovery and validation of reliable biomarkers for screening, therapy selection and prognosis. Standardization of preneoplastic and neoplastic lesion nomenclature, as well as surgical specimen processing and sampling, now provides reproducible and comparable research data that provide a basis for identifying and implementing early detection strategies and improving drug discovery. Advances in the understanding of next-generation sequencing, multidisciplinary care for GBC, neoadjuvant and adjuvant strategies, and novel systemic therapies including chemotherapy and immunotherapies are gradually changing the treatment paradigm and prognosis of this recalcitrant cancer.
© 2022. Springer Nature Limited.
Conflict of interest statement
Competing interests
M.J. receives research funding (to Institution) from Merck, EMD Serono, Novartis, Eli Lilly, Astra Zeneca, Genentech, Transthera, Meclun, BMS, Incyte, QED, Taiho, Servier, Oncosil, Basilea, Nucana; and to self or as advisory board/Data and safety Monitoring Board member from Incyte, Zymeworks, Mundi Pharma, Nucana, MORE health and Origimed. Peer grant funding from Department of Defenseand National Institute of Health. M.S. receives research funding (to Institution) from BMS, QED/HELSINN, Natera. The other authors (J.C.R., P.G., J.K., V.K.) declare no competing interests.
Figures
References
-
-
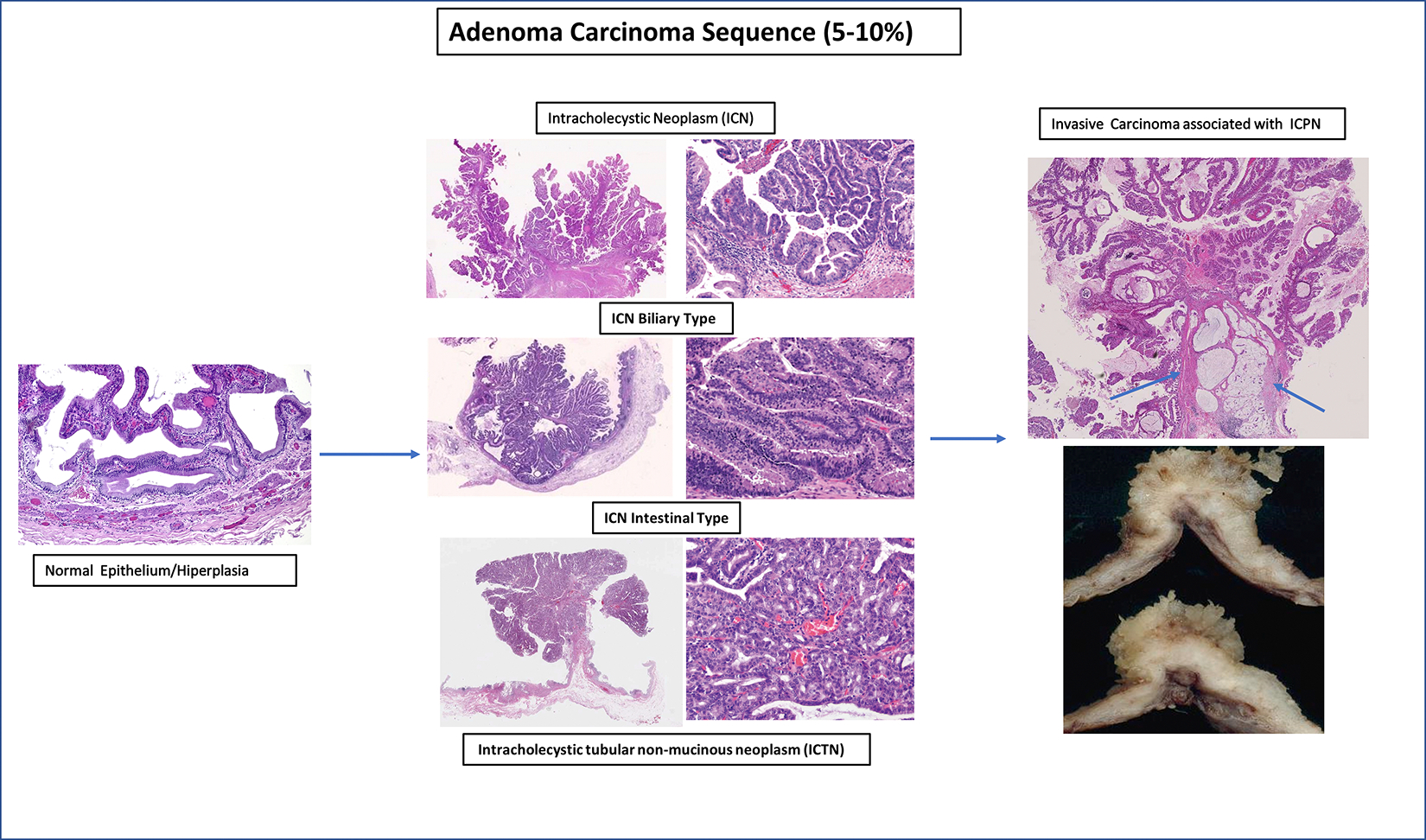
Roa JC, Basturk O & Adsay V Dysplasia and carcinoma of the gallbladder: pathological evaluation, sampling, differential diagnosis and clinical implications. Histopathology 79, 2–19, doi: 10.1111/his.14360 (2021).
Complete review that sets the basis for morphology nomenclature of preneoplastic and neoplastic gallbladder lesions.
-
-
- Roa J, Adsay NV, Arola J, Tsu W & Zen Y in Digestive System Tumours Vol. 1 WHO Classification of Tumours. (ed WHO Classification of Tumours Editorial Board; ) Ch. 9, 283–288 (IARC, 2019).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
