

IGF-2 mediated hypoglycemia and the paradox of an apparently benign lesion: a case report & review of the literature
- PMID: 36303203
- PMCID: PMC9615362
- DOI: 10.1186/s12902-022-01175-4
IGF-2 mediated hypoglycemia and the paradox of an apparently benign lesion: a case report & review of the literature
Abstract
Background: Non-islet cell tumour hypoglycemia (NICTH) is rarely encountered in clinical practice. Insulin-like growth factor 2 (IGF2) is the most common cause of NICTH observed in the setting of mesenchymal and epithelial neoplasia. This is a paraneoplastic syndrome caused by IGF2 activation of the insulin receptor.
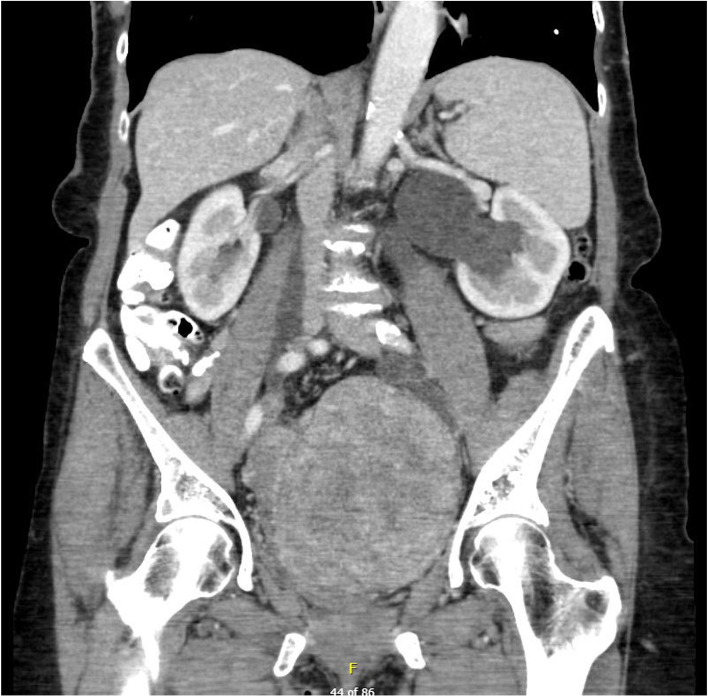
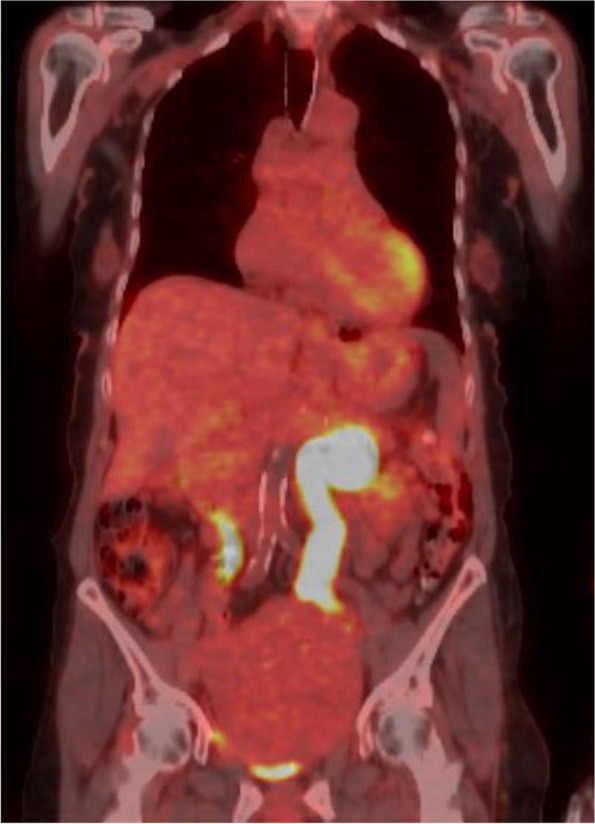
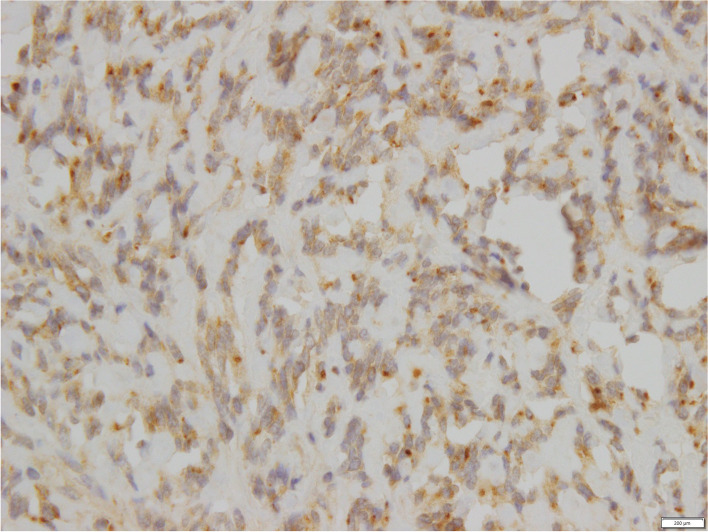
Case presentation: An 80 year old female presented with a short history of recurrent episodes of confusion with laboratory confirmed hypoglycemia with a plasma glucose of 2.7 mmol/L on fasting which fulfilled Whipple's triad. Diagnostic clues to the aetiology at presentation include the fasting pattern of hypoglycemia, hypokalaemia and the absence of weight gain. A 72 hour fast with results showed early hypoglycemia and suppression of serum insulin, c-peptide, and proinsulin. Serum insulin antibody was not detected. Subsequent measurement of the serum IGF2:IGF1 ratio was elevated at 22.3 and consistent with IGF-2 mediated hypoglycemia and imaging studies demonstrated a pelvic mass. Dietary intervention and oral prednisolone abated hypoglycemia prior to surgery. Ultimately, hypoglycemia resolved following operative intervention and steroid therapy was successfully withdrawn. Histopathology was remarkable for dual neoplastic processes with uterine solitary fibrous tumour (SFT) confirmed as the source of IGF2 hypersecretion on IGF-2 immunohistochemistry and a coincidental invasive high grade serous carcinoma involving the fimbria of the right fallopian tube.
Conclusion: The paradox in this case is that the benign solitary fibrous tumour accounted for patient morbidity through secretion of IGF2 and without treatment, posed a mortality risk. This is despite the synchronous presence of a highly malignant fallopian tube neoplasm. This case reinforces the need for thorough clinical evaluation of hypoglycemia to allow prompt and definitive management.
Keywords: Hypoglycemia; Insulin-like growth factor 2; Non-islet cell tumour hypoglycemia.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Whipple AO. The surgical therapy of hyperinsulinism. J Int Chir. 1938;3:237–276.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
