

Comparison of Whole Spine Sagittal Alignment in Patients with Spinal Disease between EOS Imaging System versus Conventional Whole Spine X-ray
- PMID: 36303311
- PMCID: PMC9629905
- DOI: 10.3349/ymj.2022.0023
Comparison of Whole Spine Sagittal Alignment in Patients with Spinal Disease between EOS Imaging System versus Conventional Whole Spine X-ray
Abstract
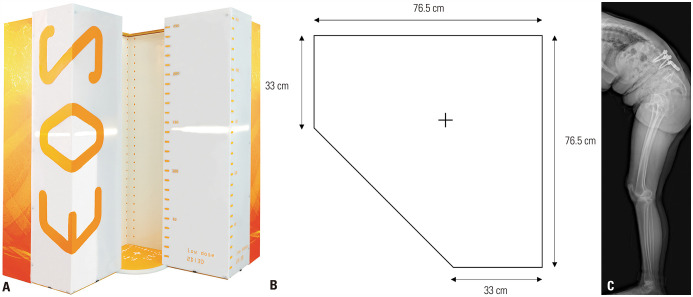
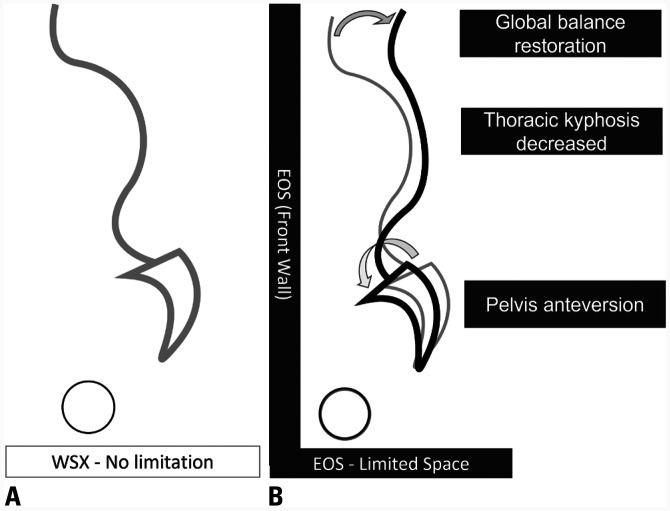
Purpose: The biplanar whole body imaging system (EOS) is a new tool for measuring the whole body sagittal alignment in a limited space. This tool may affect the sagittal balance of patients compared to conventional whole spine X-ray (WSX). This study aimed to investigate the difference in sagittal alignment between WSX and EOS.
Materials and methods: We compared the spinal and pelvic sagittal parameters in 80 patients who underwent EOS and WSX within one month between July 2018 and September 2019. The patients were divided based on sagittally balanced and imbalanced groups according to pelvic tilt (PT) >20°, pelvic incidence-lumbar lordosis >10°, C7-sagittal vertical axis (SVA) >50 mm in WSX.
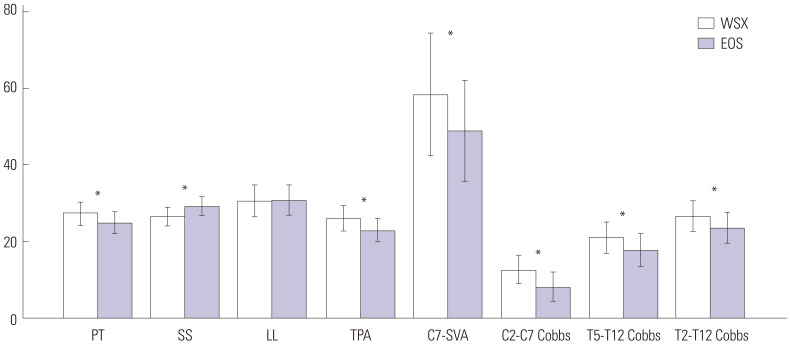
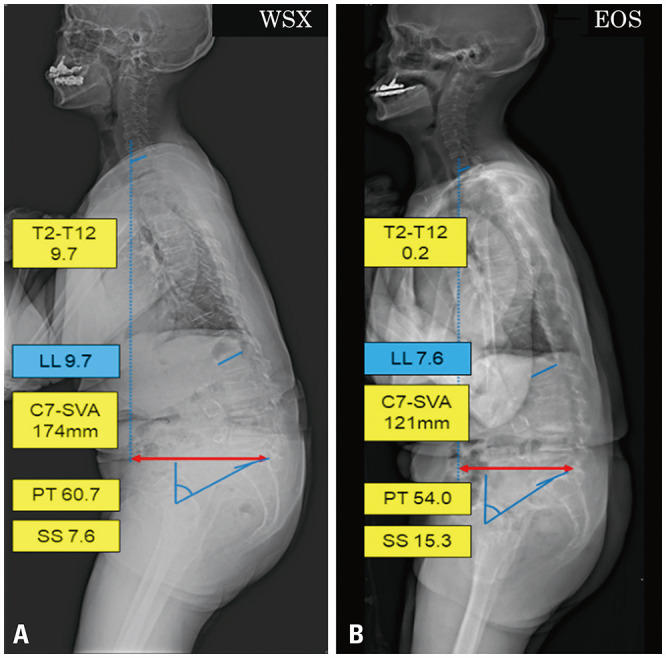
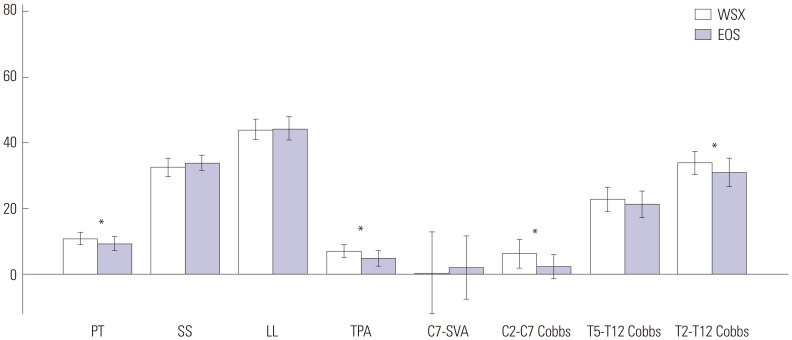
Results: In the sagittally imbalanced group, compared to WSX, the pelvic parameters demonstrated compensation in EOS with smaller PT (27.4±11.6° vs. 24.9±10.9°, p=0.003) and greater sacral slope (SS), and the patients tended to stand more upright with smaller C7-SVA (58.4±17.0 mm vs. 48.9±57.3 mm, p=0.018), T1-pelvic angle (TPA), T5-T12, and T2-T12. However, in the sagittally balanced group, these differences were less pronounced only with smaller PT (10.8±6.9° vs. 9.4±4.7°, p=0.040), TPA and T2-T12 angle, but with similar SS and C7-SVA (p>0.05).
Conclusion: EOS showed a negative SVA shift and lesser PT compared to WSX, especially in patients with sagittal imbalance. When preparing a surgical plan, surgeons should consider these differences between EOS and WSX.
Keywords: EOS; compensatory mechanism; sagittal parameters; whole spine x-ray.
© Copyright: Yonsei University College of Medicine 2022.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Characterization of Sagittal Spine Alignment With Reference to the Gravity Line and Vertebral Slopes: An Analysis of Different Roussouly Curves.Spine (Phila Pa 1976). 2020 May 1;45(9):E481-E488. doi: 10.1097/BRS.0000000000003379. Spine (Phila Pa 1976). 2020. PMID: 32282653
-
Comparison of Sagittal Spinopelvic Alignment in Patients With Ankylosing Spondylitis and Thoracolumbar Fracture.Medicine (Baltimore). 2016 Jan;95(4):e2585. doi: 10.1097/MD.0000000000002585. Medicine (Baltimore). 2016. PMID: 26825904 Free PMC article.
-
Cervical sagittal alignment in adult hyperkyphosis treated by posterior instrumentation and in situ bending.Orthop Traumatol Surg Res. 2017 Feb;103(1):53-59. doi: 10.1016/j.otsr.2016.10.003. Epub 2016 Nov 23. Orthop Traumatol Surg Res. 2017. PMID: 27889355
-
Physiological variations in the sagittal spine alignment in an asymptomatic elderly population.Spine J. 2019 Nov;19(11):1840-1849. doi: 10.1016/j.spinee.2019.07.016. Epub 2019 Aug 1. Spine J. 2019. PMID: 31377476
-
Sagittal balance of the spine.Eur Spine J. 2019 Sep;28(9):1889-1905. doi: 10.1007/s00586-019-06083-1. Epub 2019 Jul 22. Eur Spine J. 2019. PMID: 31332569 Review.
Cited by
-
Enabling technology in adult spinal deformity.Spine Deform. 2025 Apr 16. doi: 10.1007/s43390-025-01086-z. Online ahead of print. Spine Deform. 2025. PMID: 40234366 Review.
-
Spinal Injections: A Narrative Review from a Surgeon's Perspective.Healthcare (Basel). 2023 Aug 21;11(16):2355. doi: 10.3390/healthcare11162355. Healthcare (Basel). 2023. PMID: 37628553 Free PMC article. Review.
References
-
- Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976) 2005;30:2024–2029. - PubMed
-
- Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976) 2010;35:2224–2231. - PubMed
-
- Lafage V, Schwab F, Patel A, Hawkinson N, Farcy JP. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine (Phila Pa 1976) 2009;34:E599–E606. - PubMed
-
- Berjano P, Langella F, Ismael MF, Damilano M, Scopetta S, Lamartina C. Successful correction of sagittal imbalance can be calculated on the basis of pelvic incidence and age. Eur Spine J. 2014;23 Suppl 6:587–596. - PubMed
-
- Dubousset J, Charpak G, Skalli W, de Guise J, Kalifa G, Wicart P. [Skeletal and spinal imaging with EOS system] Arch Pediatr. 2008;15:665–666. French. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
