

SARS-CoV-2 specific antibody trajectories in mothers and infants over two months following maternal infection
- PMID: 36304449
- PMCID: PMC9596287
- DOI: 10.3389/fimmu.2022.1015002
SARS-CoV-2 specific antibody trajectories in mothers and infants over two months following maternal infection
Abstract
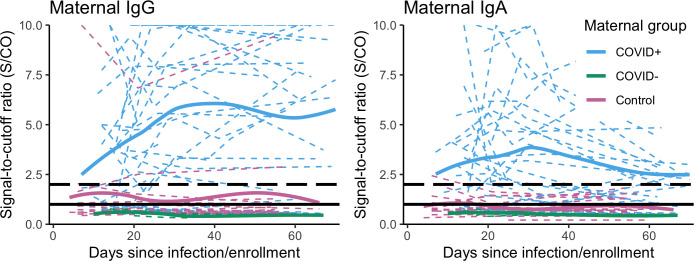
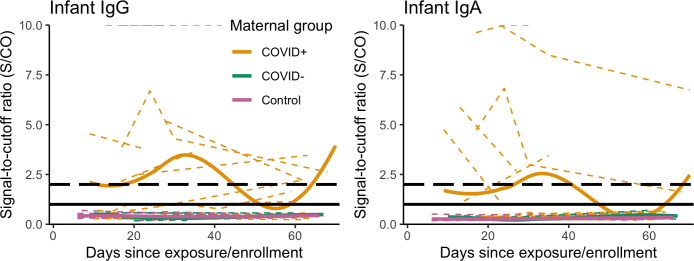
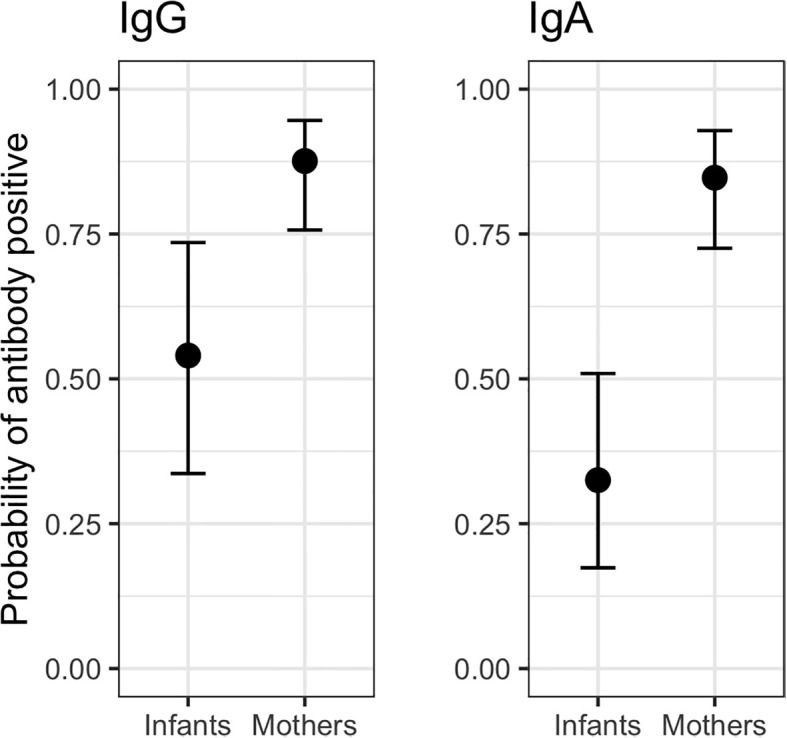
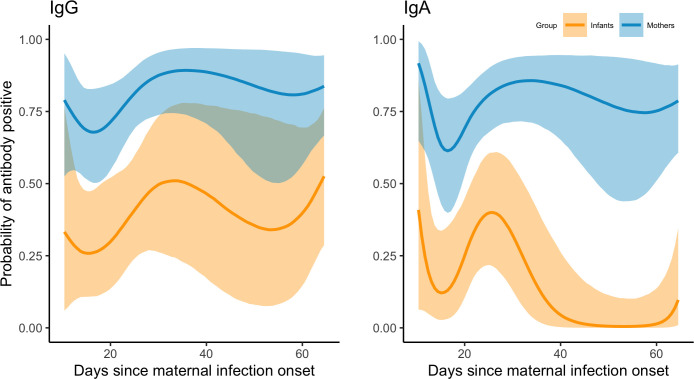
Infants exposed to caregivers infected with SARS-CoV-2 may have heightened infection risks relative to older children due to their more intensive care and feeding needs. However, there has been limited research on COVID-19 outcomes in exposed infants beyond the neonatal period. Between June 2020 - March 2021, we conducted interviews and collected capillary dried blood spots from 46 SARS-CoV-2 infected mothers and their infants (aged 1-36 months) for up to two months following maternal infection onset (COVID+ group, 87% breastfeeding). Comparative data were also collected from 26 breastfeeding mothers with no known SARS-CoV-2 infection or exposures (breastfeeding control group), and 11 mothers who tested SARS-CoV-2 negative after experiencing symptoms or close contact exposure (COVID- group, 73% breastfeeding). Dried blood spots were assayed for anti-SARS-CoV-2 S-RBD IgG and IgA positivity and anti-SARS-CoV-2 S1 + S2 IgG concentrations. Within the COVID+ group, the mean probability of seropositivity among infant samples was lower than that of corresponding maternal samples (0.54 and 0.87, respectively, for IgG; 0.33 and 0.85, respectively, for IgA), with likelihood of infant infection positively associated with the number of maternal symptoms and other household infections reported. COVID+ mothers reported a lower incidence of COVID-19 symptoms among their infants as compared to themselves and other household adults, and infants had similar PCR positivity rates as other household children. No samples returned by COVID- mothers or their infants tested antibody positive. Among the breastfeeding control group, 44% of mothers but none of their infants tested antibody positive in at least one sample. Results support previous research demonstrating minimal risks to infants following maternal COVID-19 infection, including for breastfeeding infants.
Keywords: COVID-19; IgA; IgG; breastfeeding; infancy; pediatric.
Copyright © 2022 Martin, Keith, Pace, Williams, Ley, Barbosa-Leiker, Caffé, Smith, Kunkle, Lackey, Navarrete, Pace, Gogel, Eisenberg, Fehrenkamp, McGuire, McGuire, Meehan and Brindle.
Conflict of interest statement
KL is employed by Traverse Science. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Viner RM, Mytton OT, Bonell C, Melendez-Torres GJ, Ward J, Hudson L, et al. . Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults: A systematic review and meta-analysis. JAMA Pediatr (2020) 175(2):143–56. doi: 10.1001/jamapediatrics.2020.4573 - DOI - PMC - PubMed
-
- Rudan I, Adeloye D, Katikireddi SV, Murray J, Simpson C, Shah SA, et al. . The COVID-19 pandemic in children and young people during 2020-2021: Learning about clinical presentation, patterns of spread, viral load, diagnosis and treatment. J Glob Health (2021) 11:01010. doi: 10.7189/jogh.11.01010 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous