

Wearable Sensors Improve Prediction of Post-Stroke Walking Function Following Inpatient Rehabilitation
- PMID: 36304845
- PMCID: PMC9592048
- DOI: 10.1109/JTEHM.2022.3208585
Wearable Sensors Improve Prediction of Post-Stroke Walking Function Following Inpatient Rehabilitation
Abstract
Objective: A primary goal of acute stroke rehabilitation is to maximize functional recovery and help patients reintegrate safely in the home and community. However, not all patients have the same potential for recovery, making it difficult to set realistic therapy goals and to anticipate future needs for short- or long-term care. The objective of this study was to test the value of high-resolution data from wireless, wearable motion sensors to predict post-stroke ambulation function following inpatient stroke rehabilitation.
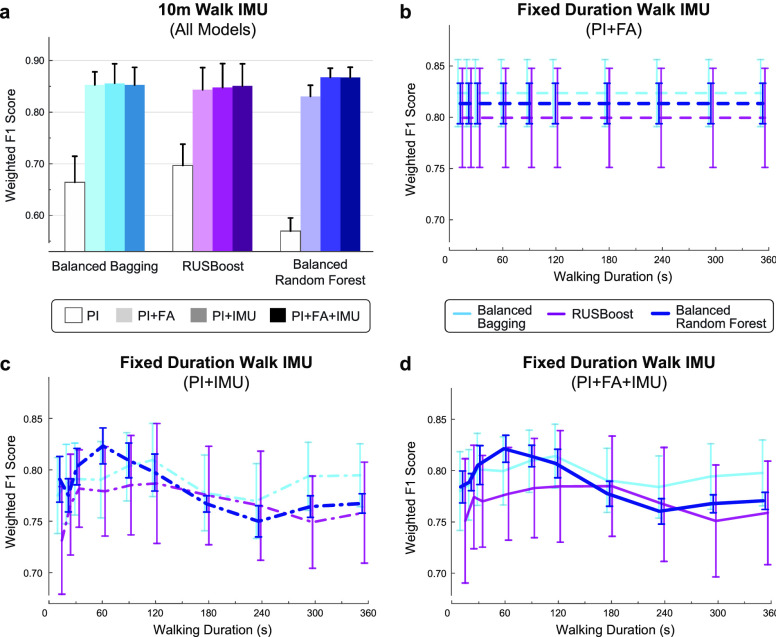
Method: Supervised machine learning algorithms were trained to classify patients as either household or community ambulators at discharge based on information collected upon admission to the inpatient facility (N=33-35). Inertial measurement unit (IMU) sensor data recorded from the ankles and the pelvis during a brief walking bout at admission (10 meters, or 60 seconds walking) improved the prediction of discharge ambulation ability over a traditional prediction model based on patient demographics, clinical information, and performance on standardized clinical assessments.
Results: Models incorporating IMU data were more sensitive to patients who changed ambulation category, improving the recall of community ambulators at discharge from 85% to 89-93%.
Conclusions: This approach demonstrates significant potential for the early prediction of post-rehabilitation walking outcomes in patients with stroke using small amounts of data from three wearable motion sensors.
Clinical impact: Accurately predicting a patient's functional recovery early in the rehabilitation process would transform our ability to design personalized care strategies in the clinic and beyond. This work contributes to the development of low-cost, clinically-implementable prognostic tools for data-driven stroke treatment.
Keywords: Accelerometers; digital health; machine learning; stroke (medical condition); wearable sensors.
Figures









References
-
- Perry J., Garrett M., Gronley J. K., and Mulroy S. J., “Classification of walking handicap in the stroke population,” Stroke, vol. 26, no. 6, pp. 982–989, Jun. 1995. - PubMed
-
- Michael K. M., Allen J. K., and Macko R. F., “Reduced ambulatory activity after stroke: The role of balance, gait, and cardiovascular fitness,” Arch. Phys. Med. Rehabil., vol. 86, no. 8, pp. 1552–1556, Aug. 2005. - PubMed
-
- Akulwar I. S., “Impact of cognitive impairments on functional ambulation in stroke patients,” Int. J. Phys. Med. Rehabil., vol. 7, no. 528, p. 2, 2019.
-
- Granger C. V., Markello S. J., Graham J. E., Deutsch A., and Ottenbacher K. J., “The uniform data system for medical rehabilitation: Report of patients with stroke discharged from comprehensive medical programs in 2000–2007,” Amer. J. Phys. Med. Rehabil., vol. 88, no. 12, pp. 961–972, Dec. 2009. - PubMed
-
- Buntin M. B.et al., “Inpatient rehabilitation facility care use before and after implementation of the IRF prospective payment system,” RAND Corp., Santa Monica, CA, USA, Tech. Rep. TR-257-CMS, 2006. Accessed: Sep. 19, 2022. [Online]. Available: https://www.rand.org/pubs/technical_reports/TR257.html
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
