

Low-frequency pre-treatment HIV drug resistance: effects on 2-year outcome of first-line efavirenz-based antiretroviral therapy
- PMID: 36305180
- PMCID: PMC9623471
- DOI: 10.1097/QAD.0000000000003361
Low-frequency pre-treatment HIV drug resistance: effects on 2-year outcome of first-line efavirenz-based antiretroviral therapy
Abstract
Objectives: Assess the impact of pre-treatment high-frequency and low-frequency drug-resistant HIV variants on long-term outcomes of first-line efavirenz-based antiretroviral therapy (ART).
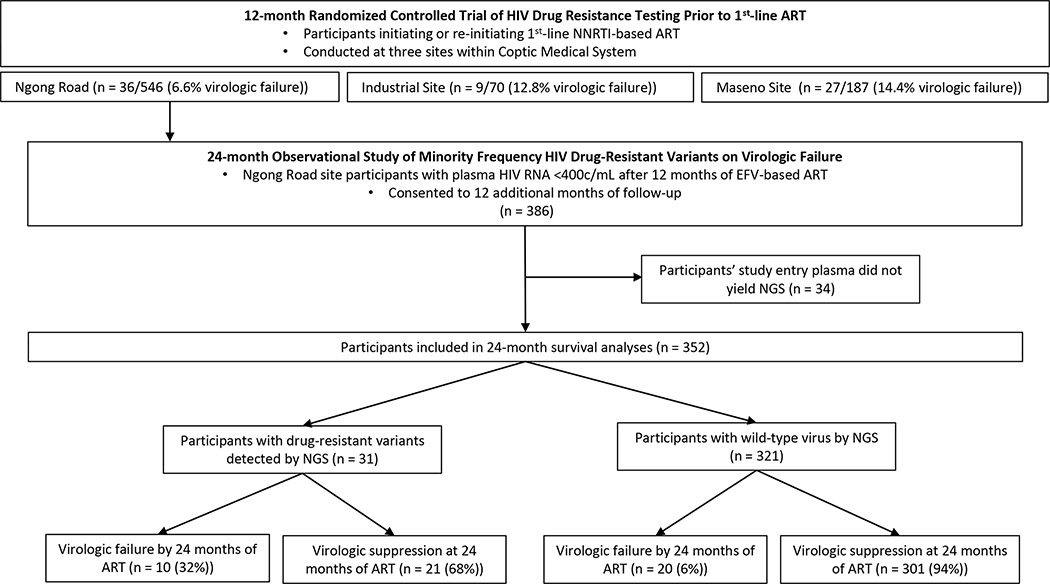
Design: Prospective observational study.
Methods: Participants' pre-treatment plasma RNA had two sections of HIV pol encoding reverse transcriptase sequenced (Illumina, MiSeq) using unique molecular identifiers to detect wild-type (pre-treatment drug-resistant variants less than 1% of viral quasispecies), low-frequency (1-9%) or high-frequency drug-resistant variants (10-100%). Associations between pre-treatment drug resistance and virologic outcomes over 24 months of efavirenz-based ART were assessed for the number and frequency of mutations by drug class and other resistance parameters.
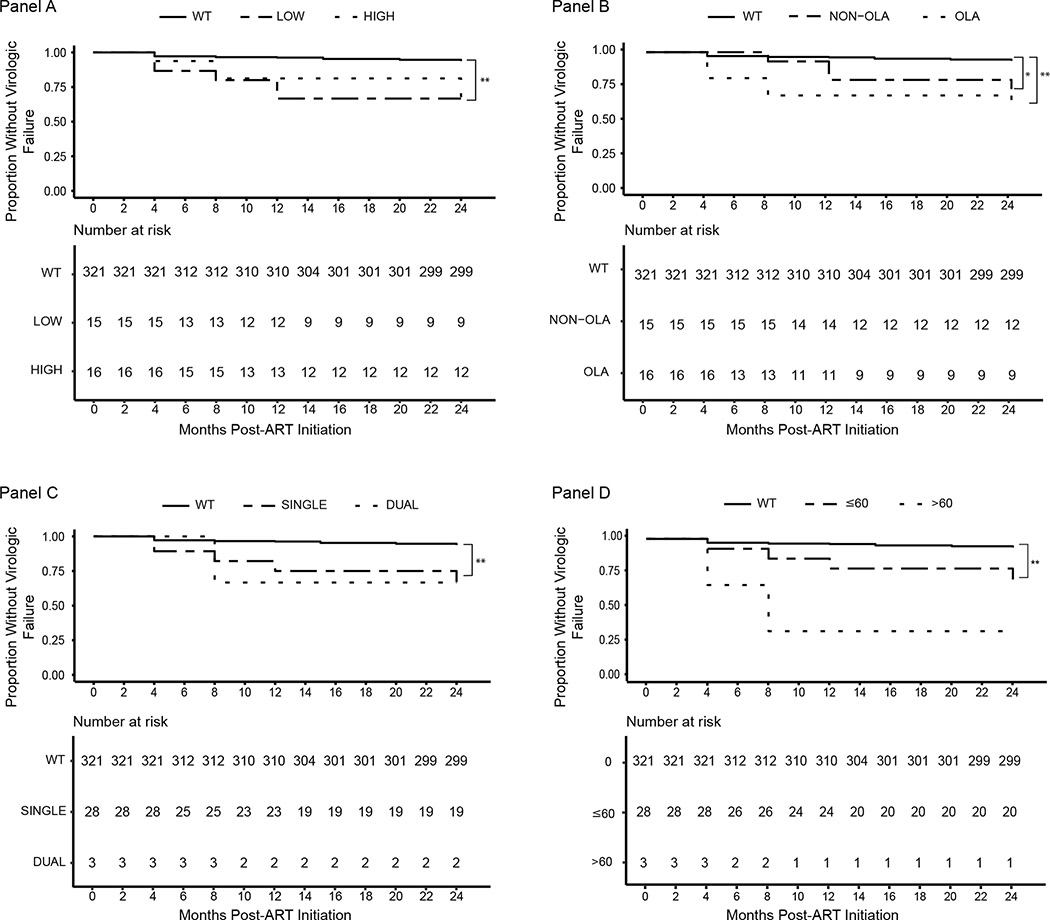
Results: Virologic failure was detected in 30 of 352 (9%) and pre-treatment drug-resistant variants were detected in the viral quasispecies of 31 of 352 (9%) participants prescribed efavirenz-based ART. Survival analyses revealed statistically significant associations between pre-treatment drug resistance at low (P < 0.0001) and high (P < 0.001) frequencies, at oligonucleotide ligation assay (OLA) (P < 0.00001) and non-OLA (P < 0.01) codons, to a single-antiretroviral class (P < 0.00001), and a shorter time to virologic failure of efavirenz-based ART. Regression analyses detected independent effects across resistance categories, including both low-frequency (P < 0.01) and high-frequency (P < 0.001) drug-resistant variants.
Conclusion: We observed that pre-treatment HIV drug resistance detected at low frequencies increased the risk of virologic failure over 24 months of efavirenz-based ART, but that most failures, regardless of drug-resistant variants' frequencies, were detected within a year of ART initiation. These observations suggest that when efavirenz-based ART is prescribed, screening for pre-treatment drug resistance by an assay capable of detecting low-frequency variants, including OLA, may guide clinicians to prescribe more effective ART.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest:
No author declared a conflict of interest.
Figures
References
-
- Gupta RK, Gregson J, Parkin N, et al. HIV-1 drug resistance before initiation or re-initiation of first-line antiretroviral therapy in low-income and middle-income countries: a systematic review and meta-regression analysis. Lancet Infect Dis. 2018;18(3):346–355. doi:10.1016/S1473-3099(17)30702-8 - DOI - PMC - PubMed
-
- Update of Recommendations on First- and Second-Line Antiretroviral Regimens. World Health Organization; 2019.
-
- Kouamou V, Mavetera J, Manasa J, et al. Pretreatment HIV Drug Resistance Among Adults Initiating or Re-Initiating First-Line Antiretroviral Therapy in Zimbabwe: Fast-Tracking the Transition to Dolutegravir-Based First-Line Regimens? AIDS Res Hum Retroviruses. 2021. Feb 5. doi: 10.1089/AID.2020.0242. Epub ahead of print. - DOI - PubMed
-
- Kantor R, Smeaton L, Vardhanabhuti S, et al. Pretreatment HIV Drug Resistance and HIV-1 Subtype C Are Independently Associated With Virologic Failure: Results From the Multinational PEARLS (ACTG A5175) Clinical Trial. Clin Infect Dis Off Publ Infect Dis Soc Am. 2015;60(10):1541–1549. doi:10.1093/cid/civ102 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
