

XEN® implantation: an effective strategy to stop glaucoma progression despite prior minimally invasive glaucoma surgery
- PMID: 36305910
- PMCID: PMC9614765
- DOI: 10.1007/s00417-022-05872-7
XEN® implantation: an effective strategy to stop glaucoma progression despite prior minimally invasive glaucoma surgery
Abstract
Purpose: The aim of this study was to evaluate whether XEN® implantation is a reasonable and safe method to lower the intraocular pressure (IOP) and amount of medication for adult primary open-angle glaucoma (POAG) over a 3-year period. The influence of the type of anesthesia, previous glaucoma surgery, and postoperative interventions on the outcome were examined.
Methods: In this retrospective study, 96 eyes were included. XEN® implantation was performed as sole procedure under general (n = 86) or local anesthesia (n = 10). IOP and number of glaucoma medication were assessed preoperatively: day 1, week 6, month 3, 6, 12, 24, and 36. Further outcome parameters were Kaplan-Meier success rates, secondary intervention, and complication rates.
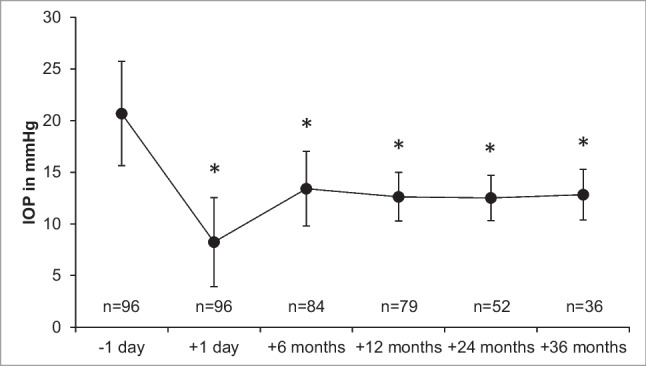
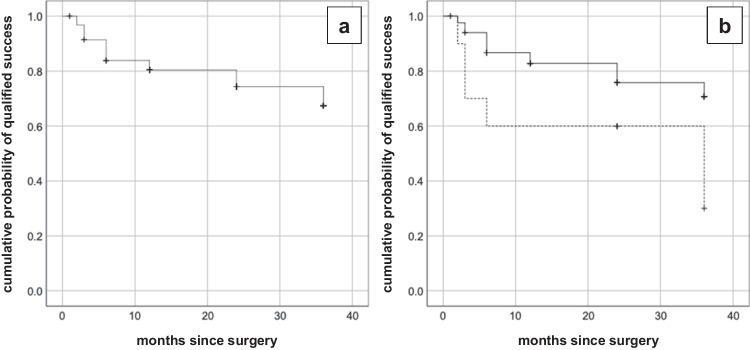
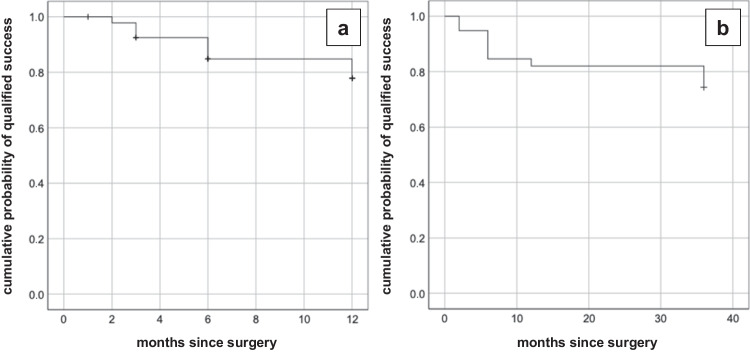
Results: IOP decreased from 20.7 ± 5.1 to 12.8 ± 2.5 mmHg at the 36-month follow-up (p < 0.001) and glaucoma therapy was reduced from 3.3 ± 0.8 to 1.2 ± 1.6 (36 months, p < 0.001). Transient postoperative hypotony was documented in 26 eyes (27.1%). General anesthesia resulted in a significant improvement of the survival rate compared to local anesthesia (77% vs. 50%, p = 0.044). Prior iStent inject®, Trabectome®, or SLT laser had no significant impact, such as filter bleb revision. The number of postoperative needlings had a significantly negative influence (p = 0.012).
Conclusion: XEN® implantation effectively and significantly lowers the IOP and number of glaucoma therapy in POAG in the 36-month follow-up with a favorable profile of side effects and few complications. In case of IOP, general anesthesia has a significant positive influence on the survival rate, whereas prior SLT or MIGS does not have significant impact.
Keywords: Glaucoma; MIGS; POAG; XEN® gel implant.
© 2022. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Selective Laser Trabeculoplasty Versus MIGS: Forgotten Art or First-Step Procedure in Selected Patients with Open-Angle Glaucoma.Ophthalmol Ther. 2021 Sep;10(3):509-524. doi: 10.1007/s40123-021-00347-0. Epub 2021 May 7. Ophthalmol Ther. 2021. PMID: 33963524 Free PMC article.
-
[XEN® Gel Stent for management of chronic open angle glaucoma: A review of the literature (French translation of the article)].J Fr Ophtalmol. 2019 Apr;42(4):391-403. doi: 10.1016/j.jfo.2018.10.005. Epub 2019 Mar 14. J Fr Ophtalmol. 2019. PMID: 30879831 Review. French.
-
Two-year outcomes of minimally invasive XEN Gel Stent implantation in primary open-angle and pseudoexfoliation glaucoma.Acta Ophthalmol. 2021 Jun;99(4):369-375. doi: 10.1111/aos.14627. Epub 2020 Sep 30. Acta Ophthalmol. 2021. PMID: 32996702 Free PMC article.
-
XEN® Gel Stent for management of chronic open angle glaucoma: A review of the literature.J Fr Ophtalmol. 2019 Feb;42(2):e37-e46. doi: 10.1016/j.jfo.2018.12.002. Epub 2019 Jan 22. J Fr Ophtalmol. 2019. PMID: 30683533 Review.
-
Efficacy of Needling Revision After XEN Gel Stent Implantation: A Prospective Study.J Glaucoma. 2020 Jan;29(1):11-14. doi: 10.1097/IJG.0000000000001394. J Glaucoma. 2020. PMID: 31702711
Cited by
-
Persistent Macular Choroidal Folds without Hypotony Following XEN Gel Stent Implantation: A Case Report.Korean J Ophthalmol. 2025 Apr;39(2):189-191. doi: 10.3341/kjo.2024.0111. Epub 2025 Feb 26. Korean J Ophthalmol. 2025. PMID: 40007194 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
