

Acoustic and Kinematic Assessment of Motor Speech Impairment in Patients With Suspected Four-Repeat Tauopathies
- PMID: 36306508
- PMCID: PMC9940887
- DOI: 10.1044/2022_JSLHR-22-00177
Acoustic and Kinematic Assessment of Motor Speech Impairment in Patients With Suspected Four-Repeat Tauopathies
Abstract
Purpose: The aim of this study was to use acoustic and kinematic speech measures to characterize type of motor speech impairment-apraxia of speech (AOS) versus dysarthria-in individuals with four-repeat tauopathy (4RT)-associated syndromes, including nonfluent variant primary progressive aphasia (nfvPPA), primary progressive AOS (PPAOS), corticobasal syndrome (CBS), and progressive supranuclear palsy syndrome (PSPs).
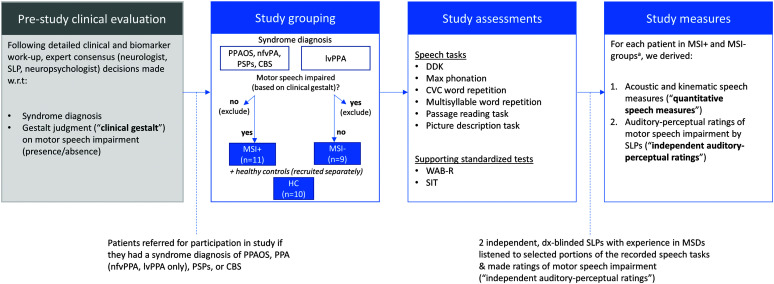
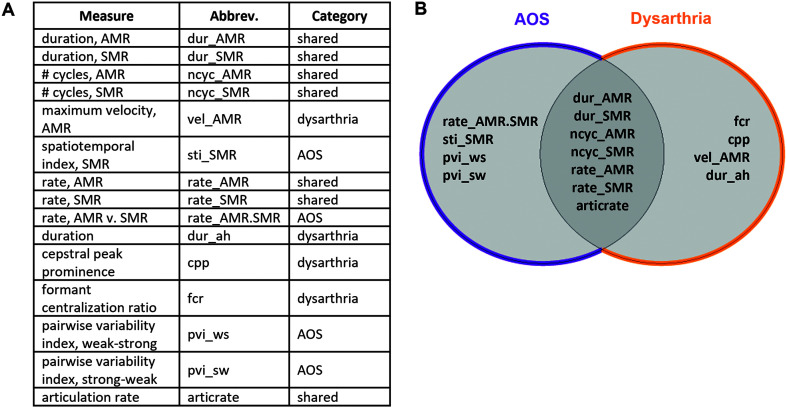
Method: Twenty patient participants were recruited and stratified into two groups: (a) a motor-speech-impaired group of individuals with nfvPPA, PPAOS, CBS, or PSPs and suspected 4RT pathology ("MSI+") and (b) a non-motor-speech-impaired group of individuals with logopenic variant primary progressive aphasia ("MSI-"). Ten healthy, age-matched controls also participated in the study. Participants completed a battery of speech tasks, and 15 acoustic and kinematic speech measures were derived. Quantitative speech measures were grouped into feature categories ("AOS features," "dysarthria features," "shared features"). In addition to quantitative speech measures, two certified speech-language pathologists made independent, blinded auditory-perceptual ratings of motor speech impairment. A principal component analysis (PCA) was conducted to investigate the relative contributions of quantitative features.
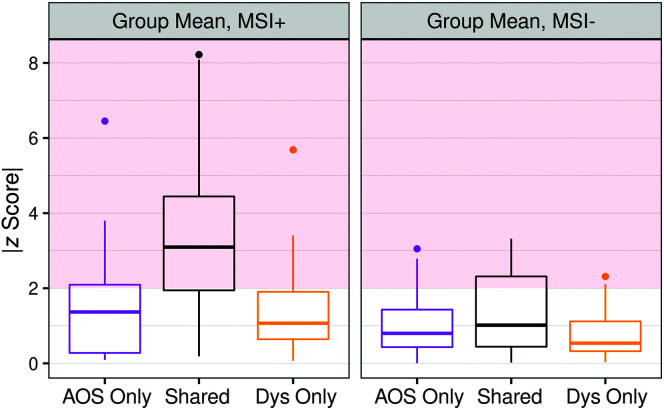
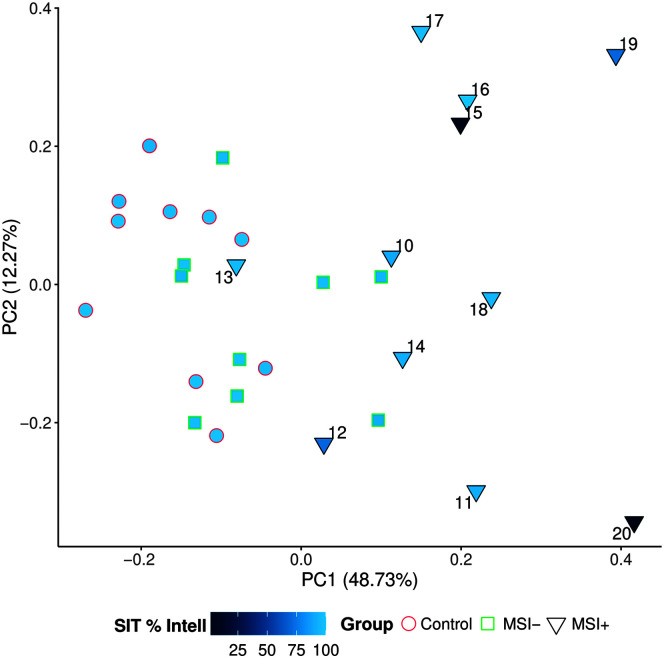
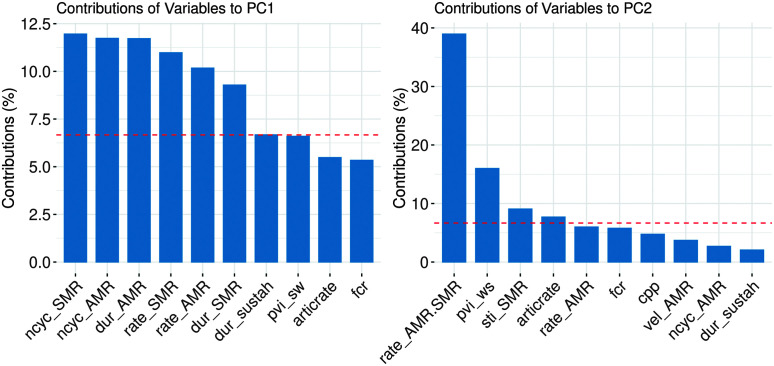
Results: Quantitative speech measures were generally concordant with independent clinician ratings of motor speech impairment severity. Hypothesis-driven groupings of quantitative measures differentiated predominantly apraxic from predominantly dysarthric presentations within the MSI+ group. PCA results provided additional evidence for differential profiles of motor speech impairment in the MSI+ group; heterogeneity across individuals is explained in large part by varying levels of overall severity-captured by the shared feature variable group-and degree of apraxia severity, as measured by the AOS feature variable group.
Conclusions: Quantitative features reveal heterogeneity of MSI in the 4RT group in terms of both overall severity and subtype of MSI. Results suggest the potential for acoustic and kinematic speech assessment methods to inform characterization of motor speech impairment in 4RT-associated syndromes.
Supplemental material: https://doi.org/10.23641/asha.21401778.
Figures
Similar articles
-
Clinical dimensions along the non-fluent variant primary progressive aphasia spectrum.Brain. 2024 Apr 4;147(4):1511-1525. doi: 10.1093/brain/awad396. Brain. 2024. PMID: 37988272 Free PMC article.
-
Neural basis of speech and grammar symptoms in non-fluent variant primary progressive aphasia spectrum.Brain. 2024 Feb 1;147(2):607-626. doi: 10.1093/brain/awad327. Brain. 2024. PMID: 37769652 Free PMC article.
-
A Longitudinal Evaluation of Speech Rate in Primary Progressive Apraxia of Speech.J Speech Lang Hear Res. 2021 Feb 17;64(2):392-404. doi: 10.1044/2020_JSLHR-20-00253. Epub 2021 Jan 21. J Speech Lang Hear Res. 2021. PMID: 33476188 Free PMC article.
-
Progressive nonfluent aphasia and its characteristic motor speech deficits.Alzheimer Dis Assoc Disord. 2007 Oct-Dec;21(4):S23-30. doi: 10.1097/WAD.0b013e31815d19fe. Alzheimer Dis Assoc Disord. 2007. PMID: 18090419 Review.
-
An Update on Apraxia of Speech.Curr Neurol Neurosci Rep. 2023 Jul;23(7):353-359. doi: 10.1007/s11910-023-01275-1. Epub 2023 Jun 3. Curr Neurol Neurosci Rep. 2023. PMID: 37269450 Free PMC article. Review.
Cited by
-
Longitudinal characterization of patients with progressive apraxia of speech without clearly predominant phonetic or prosodic speech features.Brain Lang. 2023 Oct;245:105314. doi: 10.1016/j.bandl.2023.105314. Epub 2023 Aug 20. Brain Lang. 2023. PMID: 37607419 Free PMC article.
-
Schlieren imaging and video classification of alphabet pronunciations: exploiting phonetic flows for speech recognition and speech therapy.Vis Comput Ind Biomed Art. 2024 May 22;7(1):12. doi: 10.1186/s42492-024-00163-w. Vis Comput Ind Biomed Art. 2024. PMID: 38772963 Free PMC article.
-
Connected Speech Fluency in Poststroke and Progressive Aphasia: A Scoping Review of Quantitative Approaches and Features.Am J Speech Lang Pathol. 2024 Jul 3;33(4):2091-2128. doi: 10.1044/2024_AJSLP-23-00208. Epub 2024 Apr 23. Am J Speech Lang Pathol. 2024. PMID: 38652820 Free PMC article.
References
-
- Allison, K. M. , Cordella, C. , Iuzzini-Seigel, J. , & Green, J. R. (2020). Differential diagnosis of apraxia of speech in children and adults: A scoping review. Journal of Speech, Language, and Hearing Research, 63(9), 2952–2994. https://doi.org/10.1044/2020_JSLHR-20-00061 - PMC - PubMed
-
- Allison, K. M. , Yunusova, Y. , Campbell, T. F. , Wang, J. , Berry, J. D. , & Green, J. R. (2017). The diagnostic utility of patient-report and speech-language pathologists' ratings for detecting the early onset of bulbar symptoms due to ALS. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration, 18(5–6), 358–366. https://doi.org/10.1080/21678421.2017.1303515 - PMC - PubMed
-
- Armstrong, M. J. , Litvan, I. , Lang, A. E. , Bak, T. H. , Bhatia, K. P. , Borroni, B. , Boxer, A. L. , Dickson, D. W. , Grossman, M. , Hallett, M. , Josephs, K. A. , Kertesz, A. , Lee, S. E. , Miller, B. L. , Reich, S. G. , Riley, D. E. , Tolosa, E. , Tröster, A. I. , Vidailhet, M. , & Weiner, W. J. (2013). Criteria for the diagnosis of corticobasal degeneration. Neurology, 80(5), 496–503. https://doi.org/10.1212/WNL.0b013e31827f0fd1 - PMC - PubMed
-
- Ash, S. , Evans, E. , O'Shea, J. , Powers, J. , Boller, A. , Weinberg, D. , Haley, J. , McMillan, C. , Irwin, D. J. , & Rascovsky, K. (2013). Differentiating primary progressive aphasias in a brief sample of connected speech. Neurology, 81(4), 329–336. https://doi.org/10.1212/WNL.0b013e31829c5d0e - PMC - PubMed
-
- Ballard, K. J. , Savage, S. , Leyton, C. E. , Vogel, A. P. , Hornberger, M. , & Hodges, J. R. (2014). Logopenic and nonfluent variants of primary progressive aphasia are differentiated by acoustic measures of speech production. PLOS ONE, 9(2), e89864. https://doi.org/10.1371/journal.pone.0089864 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
