

Rates of repeated colonoscopies to clean the colon from low-risk and high-risk adenomas: results from the EPoS trials
- PMID: 36307178
- PMCID: PMC11112405
- DOI: 10.1136/gutjnl-2022-327696
Rates of repeated colonoscopies to clean the colon from low-risk and high-risk adenomas: results from the EPoS trials
Abstract
Objective: High-quality colonoscopy (adequate bowel preparation, whole-colon visualisation and removal of all neoplastic polyps) is a prerequisite to start polyp surveillance, and is ideally achieved in one colonoscopy. In a large multinational polyp surveillance trial, we aimed to investigate clinical practice variation in number of colonoscopies needed to enrol patients with low-risk and high-risk adenomas in polyp surveillance.
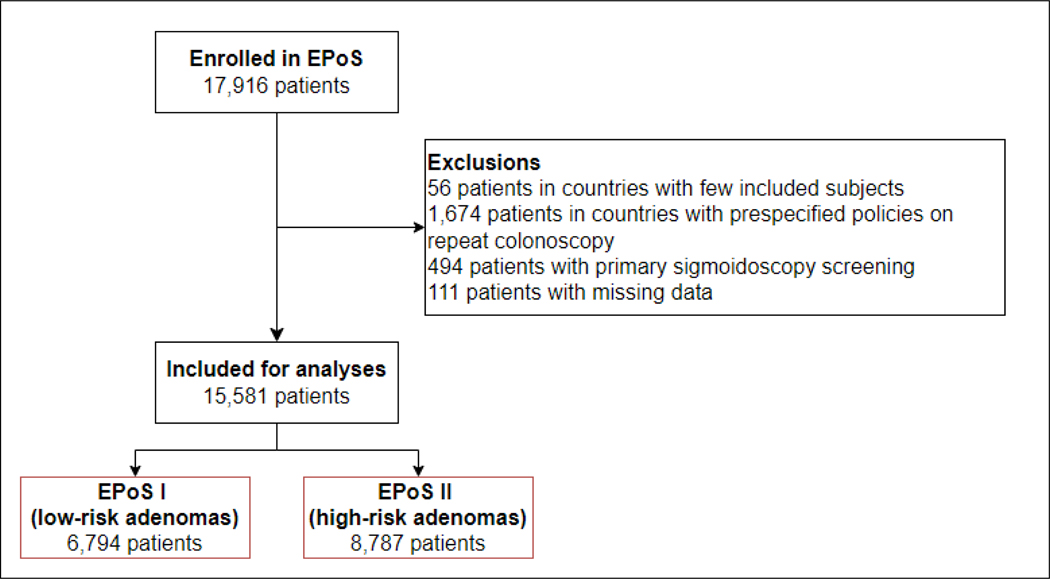
Design: We retrieved data of all patients with low-risk adenomas (one or two tubular adenomas <10 mm with low-grade dysplasia) and high-risk adenomas (3-10 adenomas, ≥1 adenoma ≥10 mm, high-grade dysplasia or villous components) in the European Polyp Surveillance trials fulfilling certain logistic and methodologic criteria. We analysed variations in number of colonoscopies needed to achieve high-quality colonoscopy and enter polyp surveillance by endoscopy centre, and by endoscopists who enrolled ≥30 patients.
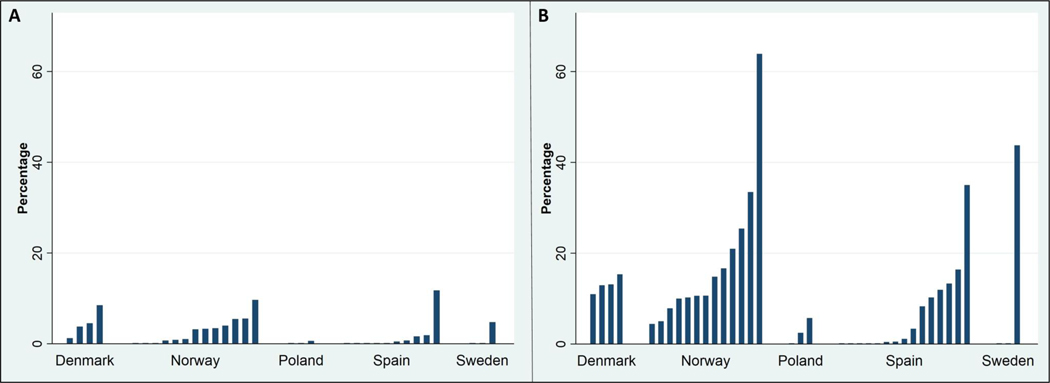
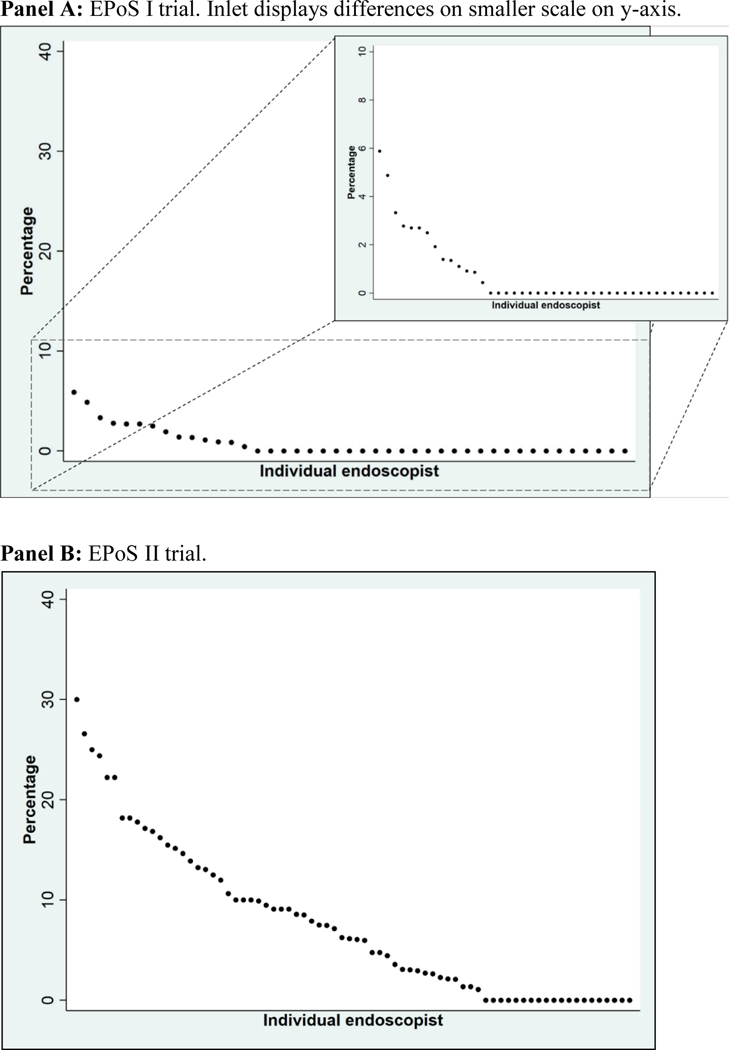
Results: The study comprised 15 581 patients from 38 endoscopy centres in five European countries; 6794 patients had low-risk and 8787 had high-risk adenomas. 961 patients (6.2%, 95% CI 5.8% to 6.6%) underwent two or more colonoscopies before surveillance began; 101 (1.5%, 95% CI 1.2% to 1.8%) in the low-risk group and 860 (9.8%, 95% CI 9.2% to 10.4%) in the high-risk group. Main reasons were poor bowel preparation (21.3%) or incomplete colonoscopy/polypectomy (14.4%) or planned second procedure (27.8%). Need of repeat colonoscopy varied between study centres ranging from 0% to 11.8% in low-risk adenoma patients and from 0% to 63.9% in high-risk adenoma patients. On the second colonoscopy, the two most common reasons for a repeat (third) colonoscopy were piecemeal resection (26.5%) and unspecified reason (23.9%).
Conclusion: There is considerable practice variation in the number of colonoscopies performed to achieve complete polyp removal, indicating need for targeted quality improvement to reduce patient burden.
Trial registration number: NCT02319928.
Keywords: COLONOSCOPY; ENDOSCOPIC POLYPECTOMY; POLYP; SURVEILLANCE.
© Author(s) (or their employer(s)) 2023. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Kaminski MF, Thomas-Gibson S, Bugajski M, et al. Performance measures for lower gastrointestinal endoscopy: a European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Endoscopy 2017;49(4):378–97. doi: 10.1055/s-0043-103411 [published Online First: 2017/03/08] - DOI - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical