

Pectus excavatum in motion: dynamic evaluation using real-time MRI
- PMID: 36307555
- PMCID: PMC9935721
- DOI: 10.1007/s00330-022-09197-1
Pectus excavatum in motion: dynamic evaluation using real-time MRI
Abstract
Objectives: The breathing phase for the determination of thoracic indices in patients with pectus excavatum is not standardized. The aim of this study was to identify the best period for reliable assessments of morphologic indices by dynamic observations of the chest wall using real-time MRI.
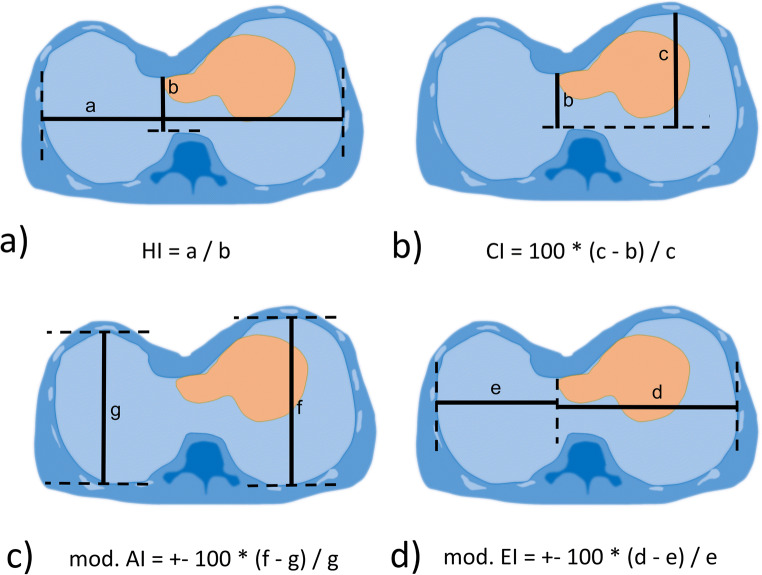
Methods: In this prospective study, patients with pectus excavatum underwent morphologic evaluation by real-time MRI at 3 T between January 2020 and June 2021. The Haller index (HI), correction index (CI), modified asymmetry index (AI), and modified eccentricity index (EI) were determined during free, quiet, and forced breathing respectively. Breathing-related differences in the thoracic indices were analyzed with the Wilcoxon signed-rank test. Motion of the anterior chest wall was analyzed as well.
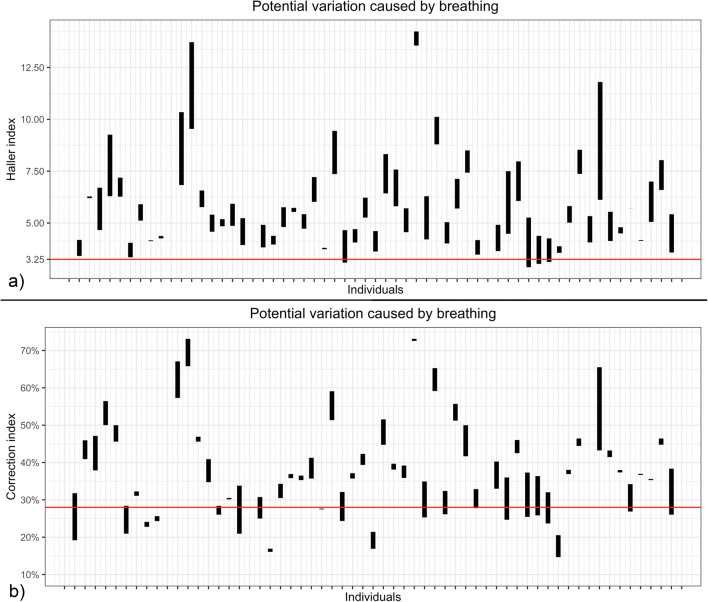
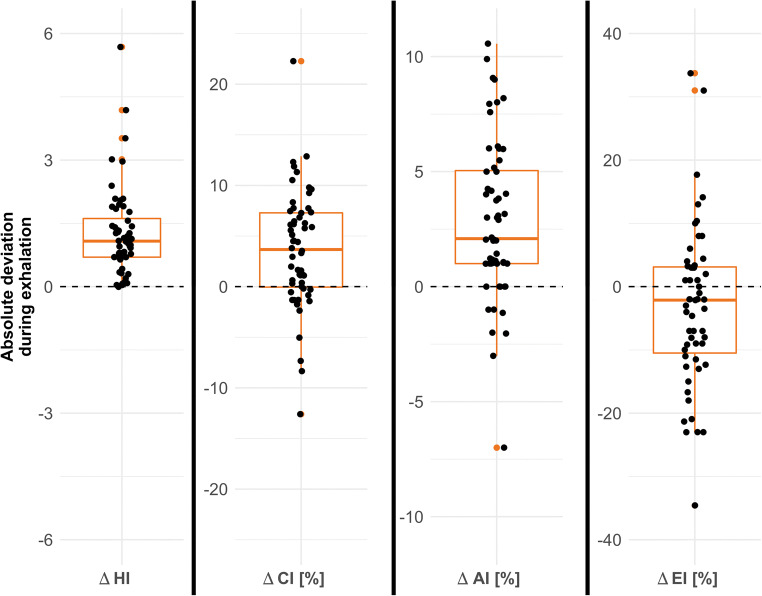
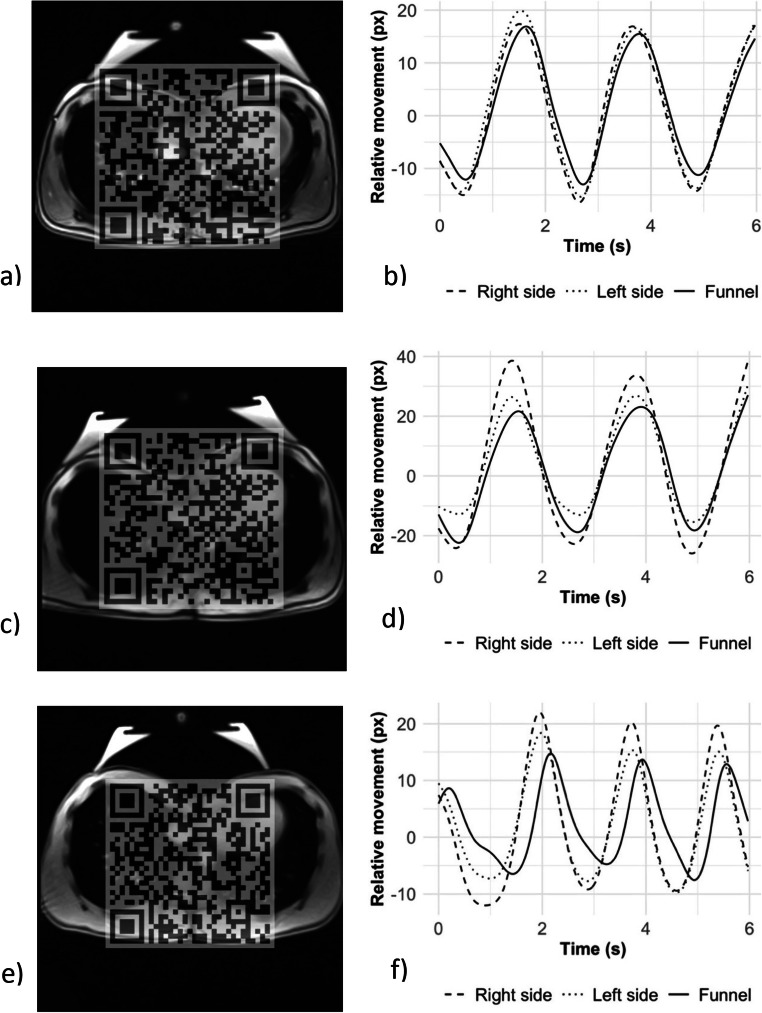
Results: A total of 56 patients (11 females and 45 males, median age 15.4 years, interquartile range 14.3-16.9) were included. In quiet expiration, the median HI in the cohort equaled 5.7 (4.5-7.2). The median absolute differences (Δ) in the thoracic indices between peak inspiration and peak expiration were ΔHI = 1.1 (0.7-1.6, p < .001), ΔCI = 4.8% (1.3-7.5%, p < .001), ΔAI = 3.0% (1.0-5.0%, p < .001), and ΔEI = 8.0% (3.0-14.0%, p < .05). The indices varied significantly during different inspiratory phases, but not during expiration (p > .05 each). Furthermore, the dynamic evaluation revealed three distinctive movement patterns of the funnel chest.
Conclusions: Real-time MRI reveals patterns of chest wall motion and indicate that thoracic indices of pectus excavatum should be assessed in the end-expiratory phase of quiet expiration.
Key points: • The thoracic indices in patients with pectus excavatum depend on the breathing phase. • Quiet expiration represents the best breathing phase for determining thoracic indices. • Real-time MRI can identify different chest wall motion patterns in pectus excavatum.
Keywords: Funnel chest; Magnetic resonance imaging; Thoracic wall.
© 2022. The Author(s).
Conflict of interest statement
Jens Frahm and Dirk Voit are co-inventors of a patent and software describing the real-time MRI technique used here for real-time MR imaging. The other authors declare no competing interests
Figures
Similar articles
-
Advancements in preoperative imaging of pectus excavatum: a comprehensive review.J Thorac Dis. 2024 Jan 30;16(1):696-707. doi: 10.21037/jtd-23-662. Epub 2024 Jan 24. J Thorac Dis. 2024. PMID: 38410537 Free PMC article. Review.
-
Morphologic assessment of thoracic deformities for the preoperative evaluation of pectus excavatum by magnetic resonance imaging.Eur Radiol. 2015 Mar;25(3):785-91. doi: 10.1007/s00330-014-3450-0. Epub 2014 Oct 15. Eur Radiol. 2015. PMID: 25316056
-
Changes in chest compression indexes with breathing underestimate surgical candidacy in patients with pectus excavatum: a computed tomography pilot study.J Pediatr Surg. 2013 Oct;48(10):2011-6. doi: 10.1016/j.jpedsurg.2013.01.044. J Pediatr Surg. 2013. PMID: 24094949
-
Comparison of Haller index values calculated with chest radiographs versus CT for pectus excavatum evaluation.Pediatr Radiol. 2010 Nov;40(11):1763-7. doi: 10.1007/s00247-010-1681-z. Epub 2010 May 15. Pediatr Radiol. 2010. PMID: 20473605
-
Quantification of pectus excavatum: Anatomic indices.Semin Pediatr Surg. 2018 Jun;27(3):122-126. doi: 10.1053/j.sempedsurg.2018.05.006. Epub 2018 May 16. Semin Pediatr Surg. 2018. PMID: 30078482 Review.
Cited by
-
Real-time MRI: a new tool of radiologic imaging in small children.Eur J Pediatr. 2023 Aug;182(8):3405-3417. doi: 10.1007/s00431-023-04996-0. Epub 2023 May 30. Eur J Pediatr. 2023. PMID: 37249681 Free PMC article. Review.
-
Functional and Aesthetic Outcomes of Patients Underwent Modified Ravitch Technique for Repair of Pectus Excavatum.Med J Islam Repub Iran. 2024 Aug 20;38:95. doi: 10.47176/mjiri.38.95. eCollection 2024. Med J Islam Repub Iran. 2024. PMID: 39678765 Free PMC article.
-
Advancements in preoperative imaging of pectus excavatum: a comprehensive review.J Thorac Dis. 2024 Jan 30;16(1):696-707. doi: 10.21037/jtd-23-662. Epub 2024 Jan 24. J Thorac Dis. 2024. PMID: 38410537 Free PMC article. Review.
-
Initial study on an expert system for spine diseases screening using inertial measurement unit.Sci Rep. 2023 Jun 27;13(1):10440. doi: 10.1038/s41598-023-36798-7. Sci Rep. 2023. PMID: 37369726 Free PMC article.
References
-
- Steinmann C, Krille S, Mueller A, Weber P, Reingruber B, Martin A (2011) Pectus excavatum and pectus carinatum patients suffer from lower quality of life and impaired body image: a control group comparison of psychological characteristics prior to surgical correction. Eur J Cardiothorac Surg 40:1138–1145 - PubMed
