

Association of early dexamethasone therapy with mortality in critically Ill COVID-19 patients: a French multicenter study
- PMID: 36308564
- PMCID: PMC9617242
- DOI: 10.1186/s13613-022-01074-w
Association of early dexamethasone therapy with mortality in critically Ill COVID-19 patients: a French multicenter study
Abstract
Background: Dexamethasone is recommended for COVID-19 patients who require oxygen therapy. However, its effectiveness in reducing mortality and intubation, and its safety, remain debated. We aimed to investigate whether dexamethasone reduces day-28 mortality in unselected patients with critical COVID-19.
Methods: We performed an observational cohort study in consecutive COVID-19 patients admitted to any of 13 French intensive care units (ICUs) in 2020. The primary objective was to determine whether early dexamethasone therapy was associated with day-28 mortality and the secondary objectives were to assess whether early dexamethasone decreased intubation requirements and to collect adverse events.
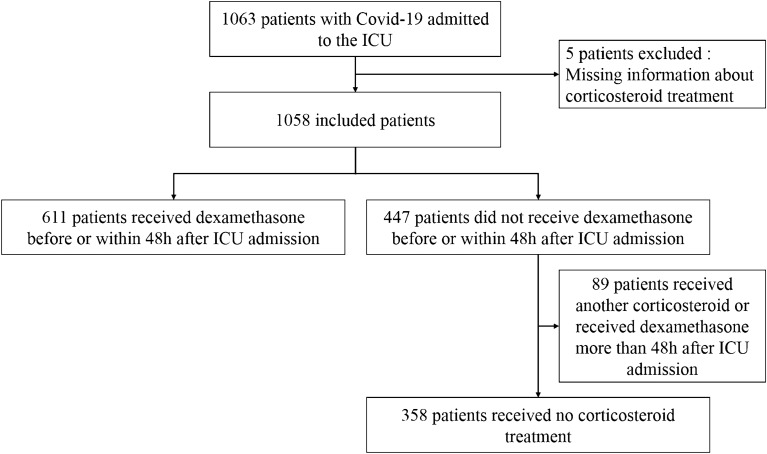
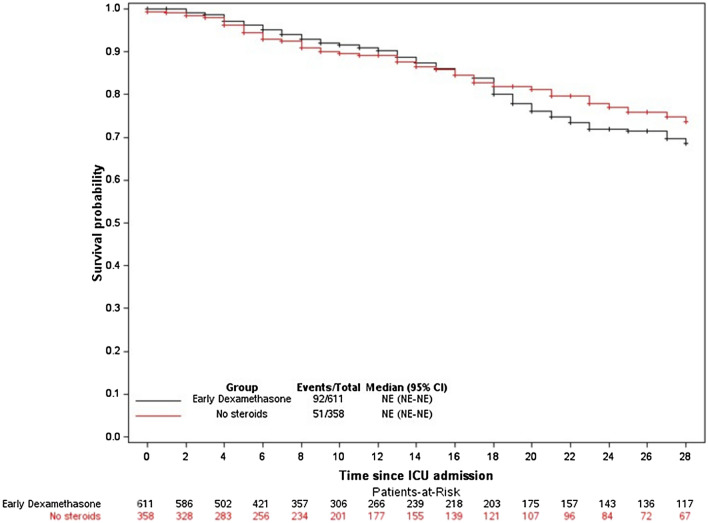
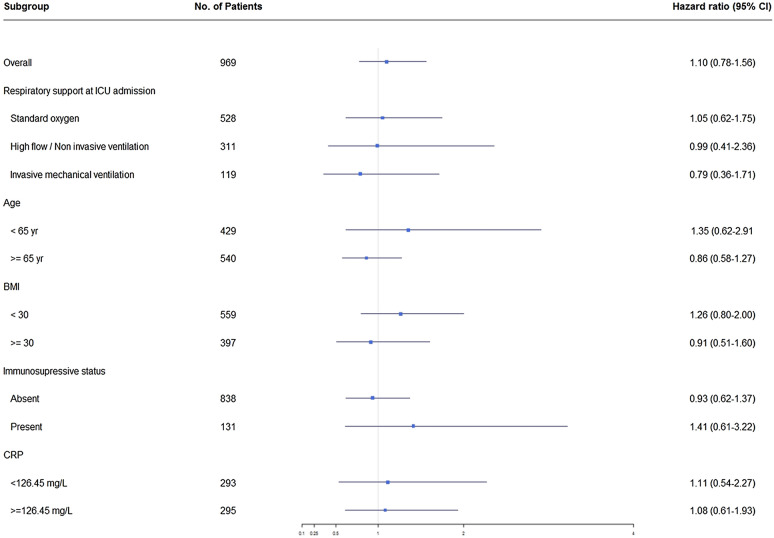
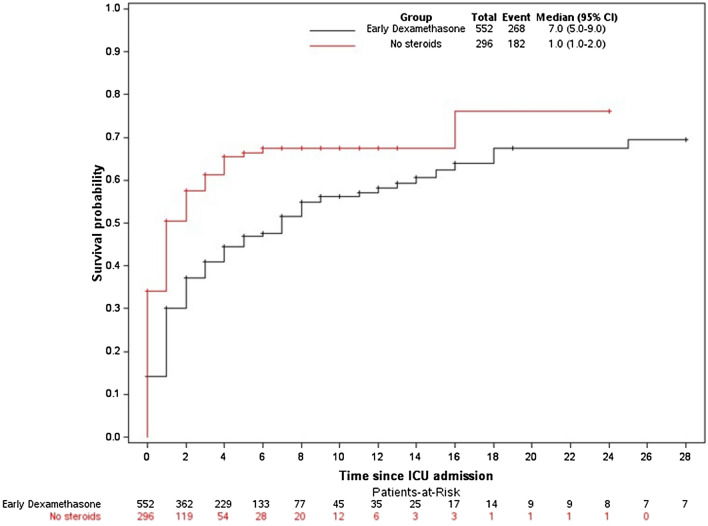
Results: Of 1058 included patients, 611 (57.75%) received early dexamethasone (early dexamethasone group), 358 (33.83%) did not receive any steroids (no steroids group), and 89 (8.41%) received late dexamethasone or other steroids. Day-28 mortality was similar between the early dexamethasone and the no steroids groups (15.06% and 14.25%, respectively; P = 0.59). Factors associated with day-28 mortality were older age (adjusted hazard ratio [aHR], 1.06; 1.04-1.09; P < 0.001), worse SOFA score (aHR, 1.13; 1.06-1.20; P < 0.001), and immunocompromised status (aHR, 1.59; 1.01-2.50; P = 0.043). Early dexamethasone was associated with fewer intubations (48.55% vs. 61.49%, P < 0.001) and more ventilator-free days by day 28 (22 [2-28] vs. 17 [1-28] days, P = 0.003), compared to no steroids. Ventilator-associated pneumonia (VAP) was more common with early dexamethasone (HR, 1.29 [1.01-1.63], P = 0.04) than with no steroids, whereas no differences were noted for bloodstream infection, fungal infection, or gastrointestinal bleeding.
Conclusions: Early dexamethasone in critically ill COVID-19 patients was not associated with lower day-28 mortality. However, early dexamethasone was associated with lower intubation needs and more ventilator-free days by day 28. In patients treated with invasive mechanical ventilation, early dexamethasone was associated with a higher risk of VAP.
Keywords: COVID-19; Dexamethasone; Intubation; Mortality; Ventilator-associated pneumonia.
© 2022. The Author(s).
Conflict of interest statement
EC has received lecturer and conference-speaker fees, as well as reimbursements of travel and accommodation expenses related to attending scientific meetings, from Gilead, Baxter, and Sanofi-Genzyme. JBL has received lecturer and conference-speaker fees from BD and Zoll. None of the other authors have any competing interests to disclose.
Figures
References
-
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html. Accessed 14 Jan 2021
-
- Corticosteroids for COVID-19. https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Corticost... Accessed 14 Jan 2021
-
- Villar, J. Efficacy of dexamethasone treatment for patients With ARDS Caused by COVID-19. clinicaltrials.gov 2021 Feb. Report No: NCT04325061. https://clinicaltrials.gov/ct2/show/NCT04325061
LinkOut - more resources
Full Text Sources
