

Adipokines: Deciphering the cardiovascular signature of adipose tissue
- PMID: 36309078
- PMCID: PMC10509780
- DOI: 10.1016/j.bcp.2022.115324
Adipokines: Deciphering the cardiovascular signature of adipose tissue
Abstract
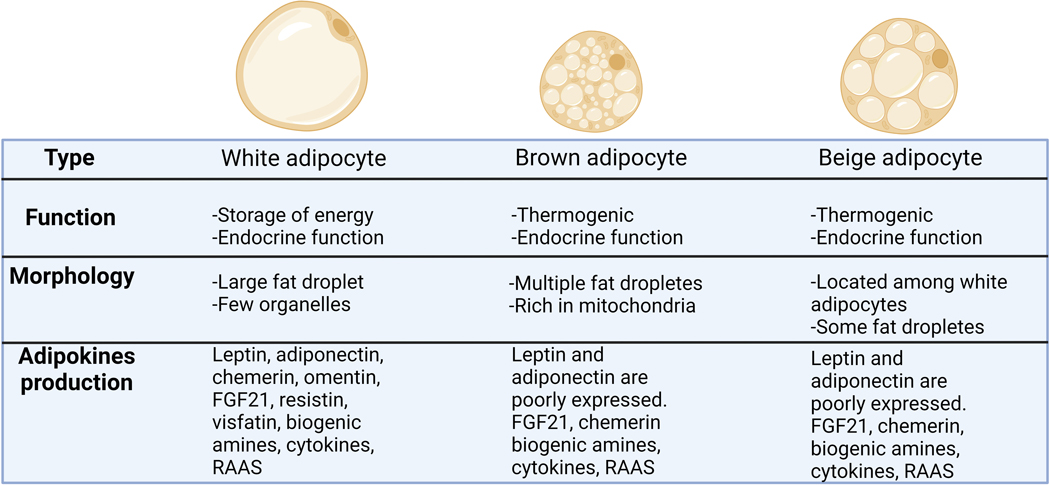
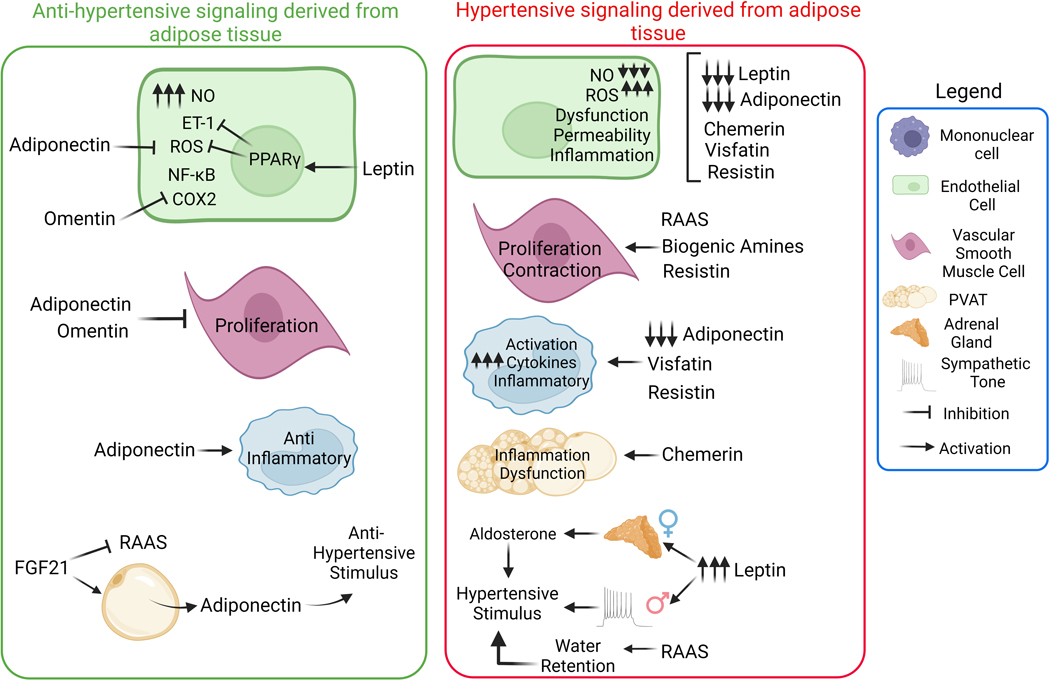
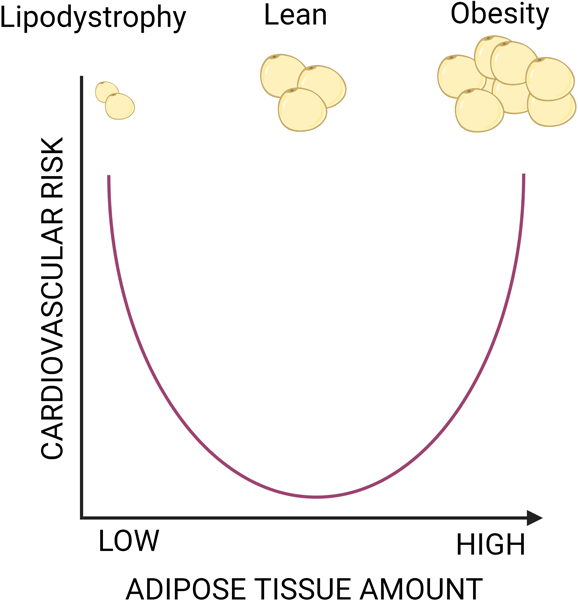
Obesity and hypertension are intimately linked due to the various ways that the important cell types such as vascular smooth muscle cells (VSMC), endothelial cells (EC), immune cells, and adipocytes, communicate with one another to contribute to these two pathologies. Adipose tissue is a very dynamic organ comprised primarily of adipocytes, which are well known for their role in energy storage. More recently adipose tissue has been recognized as the largest endocrine organ because of its ability to produce a vast number of signaling molecules called adipokines. These signaling molecules stimulate specific types of cells or tissues with many adipokines acting as indicators of adipocyte healthy function, such as adiponectin, omentin, and FGF21, which show anti-inflammatory or cardioprotective effects, acting as regulators of healthy physiological function. Others, like visfatin, chemerin, resistin, and leptin are often altered during pathophysiological circumstances like obesity and lipodystrophy, demonstrating negative cardiovascular outcomes when produced in excess. This review aims to explore the role of adipocytes and their derived products as well as the impacts of these adipokines on blood pressure regulation and cardiovascular homeostasis.
Keywords: Adipocytes; Adipose tissue; Blood pressure; Blood vessels.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Relevance of Leptin and Other Adipokines in Obesity-Associated Cardiovascular Risk.Nutrients. 2019 Nov 5;11(11):2664. doi: 10.3390/nu11112664. Nutrients. 2019. PMID: 31694146 Free PMC article. Review.
-
Regulation of vascular tone by adipocytes.BMC Med. 2011 Mar 16;9:25. doi: 10.1186/1741-7015-9-25. BMC Med. 2011. PMID: 21410966 Free PMC article. Review.
-
Adipokines and the cardiovascular system: mechanisms mediating health and disease.Can J Physiol Pharmacol. 2012 Aug;90(8):1029-59. doi: 10.1139/y2012-053. Epub 2012 May 30. Can J Physiol Pharmacol. 2012. PMID: 22646022 Review.
-
Targeting adipokines: A new strategy for the treatment of myocardial fibrosis.Pharmacol Res. 2022 Jul;181:106257. doi: 10.1016/j.phrs.2022.106257. Epub 2022 May 13. Pharmacol Res. 2022. PMID: 35569708 Review.
-
Leptin, resistin and visfatin: the missing link between endocrine metabolic disorders and immunity.Eur J Med Res. 2013 May 1;18(1):12. doi: 10.1186/2047-783X-18-12. Eur J Med Res. 2013. PMID: 23634778 Free PMC article. Review.
Cited by
-
Adipose Tissue-Derived Adipokines in Vascular Physiology and Pathophysiology: Insights and Implications.Compr Physiol. 2025 Jun;15(3):e70018. doi: 10.1002/cph4.70018. Compr Physiol. 2025. PMID: 40451771 Review.
-
Adipokines in preeclampsia: disrupted signaling pathways and novel therapeutic strategies.Eur J Med Res. 2025 Aug 4;30(1):702. doi: 10.1186/s40001-025-02972-y. Eur J Med Res. 2025. PMID: 40759967 Free PMC article. Review.
-
Chemerin in the Spotlight: Revealing Its Multifaceted Role in Acute Myocardial Infarction.Biomedicines. 2024 Sep 20;12(9):2133. doi: 10.3390/biomedicines12092133. Biomedicines. 2024. PMID: 39335646 Free PMC article. Review.
-
Cyclodextrin-Mediated Cholesterol Depletion Induces Adiponectin Secretion in 3T3-L1 Adipocytes.Int J Mol Sci. 2023 Sep 28;24(19):14718. doi: 10.3390/ijms241914718. Int J Mol Sci. 2023. PMID: 37834165 Free PMC article.
-
Could Naringenin Participate as a Regulator of Obesity and Satiety?Molecules. 2023 Feb 2;28(3):1450. doi: 10.3390/molecules28031450. Molecules. 2023. PMID: 36771113 Free PMC article. Review.
References
-
- Fain JN, Madan AK, Hiler ML, Cheema P, Bahouth SW, Comparison of the release of adipokines by adipose tissue, adipose tissue matrix, and adipocytes from visceral and subcutaneous abdominal adipose tissues of obese humans, Endocrinology 145(5) (2004) 2273–82. - PubMed
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Jordan LC, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, O’Flaherty M, Pandey A, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Spartano NL, Stokes A, Tirschwell DL, Tsao CW, Turakhia MP, VanWagner LB, Wilkins JT, Wong SS, Virani SS, Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association, Circulation 139(10) (2019) e56–e528. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr., Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr., Williamson JD, Wright JT Jr., 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, Circulation 138(17) (2018) e426–e483. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr., Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr., Williamson JD, Wright JT Jr., 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, Journal of the American College of Cardiology 71(19) (2018) e127–e248. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
