

Adherence to and impact of home-based high-intensity IMT in people with spinal cord injury: a pilot study
- PMID: 36309488
- PMCID: PMC9617741
- DOI: 10.1038/s41394-022-00551-5
Adherence to and impact of home-based high-intensity IMT in people with spinal cord injury: a pilot study
Abstract
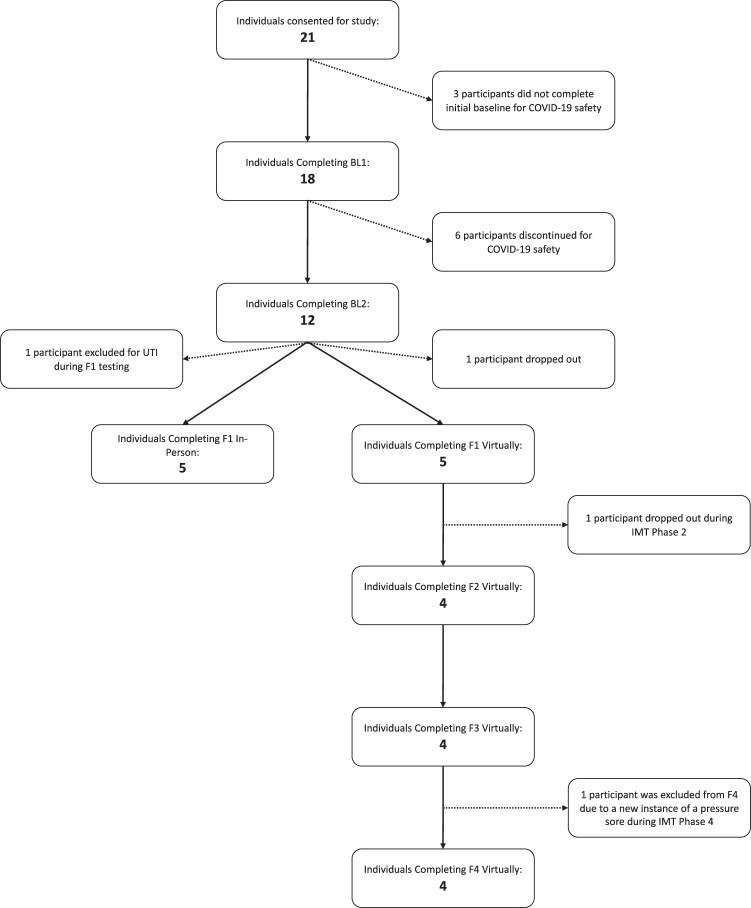
Study design: The pilot study was completed in 5 phases (Control and 4 phases of IMT) incorporating assessments at Baseline 1 (BL1), BL2, Follow-up 1 (F1), F2, F3, and F4.
Objective: To assess the adherence and impact of a daily high-intensity (80% of max) inspiratory muscle training (IMT) home program with once weekly supervision for people with spinal cord injury (SCI).
Setting: Assessments: research institution or zoom. IMT: participant's home.
Methods: Participants completed daily IMT in IMT Phase 1 and 2, once weekly in IMT Phase 3, self-selected frequency in IMT Phase 4. All phases had one weekly supervised session except IMT Phase 4. Primary outcomes included adherence and a difficulty score [DS (0- not difficult to 10- the most difficult)]. Secondary outcomes included respiratory function and seated balance.
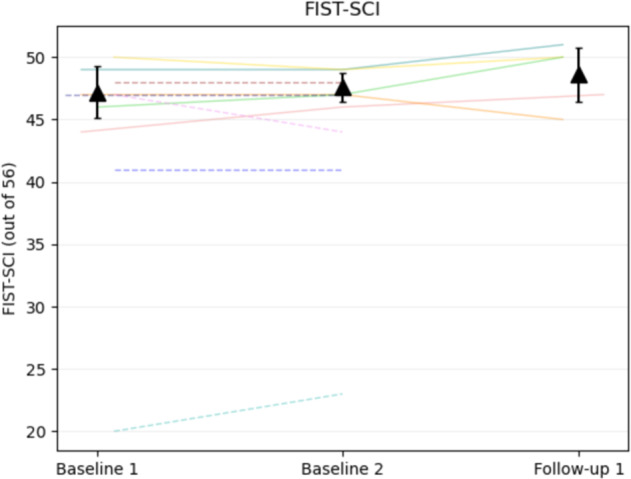
Results: Data from 10 people with chronic SCI (>1 year) (Cervical level of injury: 6, AIS: A-B, injury duration: 10.9 years 95% CI [3.9, 18.1]) were used in the analysis. Participants completed 69% of their training days in IMT Phase 1 and 65% overall reporting an average DS of 7.4 ± 1.4. Only one participant completed training during IMT Phase 4. One participant's training load was reduced due to suspected overtraining. Maximal inspiratory pressure (MIP), sustained MIP (SMIP), and total power (TP), improved significantly (p < 0.05) from BL2 to F1.
Conclusion: Our data suggest that people with SCI can perform high-intensity IMT at home to improve inspiratory performance. It is strongly recommended that participants be intermittently monitored for adherence and safety.
Clinicaltrials: gov Registration number: NCT04210063.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- Postma K, Vlemmix LY, Haisma JA, de Groot S, Sluis TA, Stam HJ, et al. Longitudinal association between respiratory muscle strength and cough capacity in persons with spinal cord injury: An explorative analysis of data from a randomized controlled trial. J Rehabil Med. 2015;47:722–6. - PubMed
-
- DeVivo MJ, Chen Y, Wen H. Cause of death trends among persons with spinal cord injury in the United States 1960-2017. Arch Phys Med Rehab. 2021;103:634–641. - PubMed
-
- Palermo AE, Janyszek E, Young A, Villane A, Kirk-Sanchez NJ, Cahalin LP, et al. Inspiratory muscle performance and anthropometric measures—novel assessments related to pulmonary function in people with spinal cord. Injury: A Pilot Study Arch Phys Med Rehab. 2022;103:441–50. - PubMed
-
- DeVivo MJ, Kartus PL, Stover SL, Rutt RD, Fine PR. Cause of death for patients with spinal cord injuries. Arch Phys Med Rehabil. 1989;149:1761–6. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
