

Single-cell profiling reveals distinct adaptive immune hallmarks in MDA5+ dermatomyositis with therapeutic implications
- PMID: 36309526
- PMCID: PMC9617246
- DOI: 10.1038/s41467-022-34145-4
Single-cell profiling reveals distinct adaptive immune hallmarks in MDA5+ dermatomyositis with therapeutic implications
Abstract
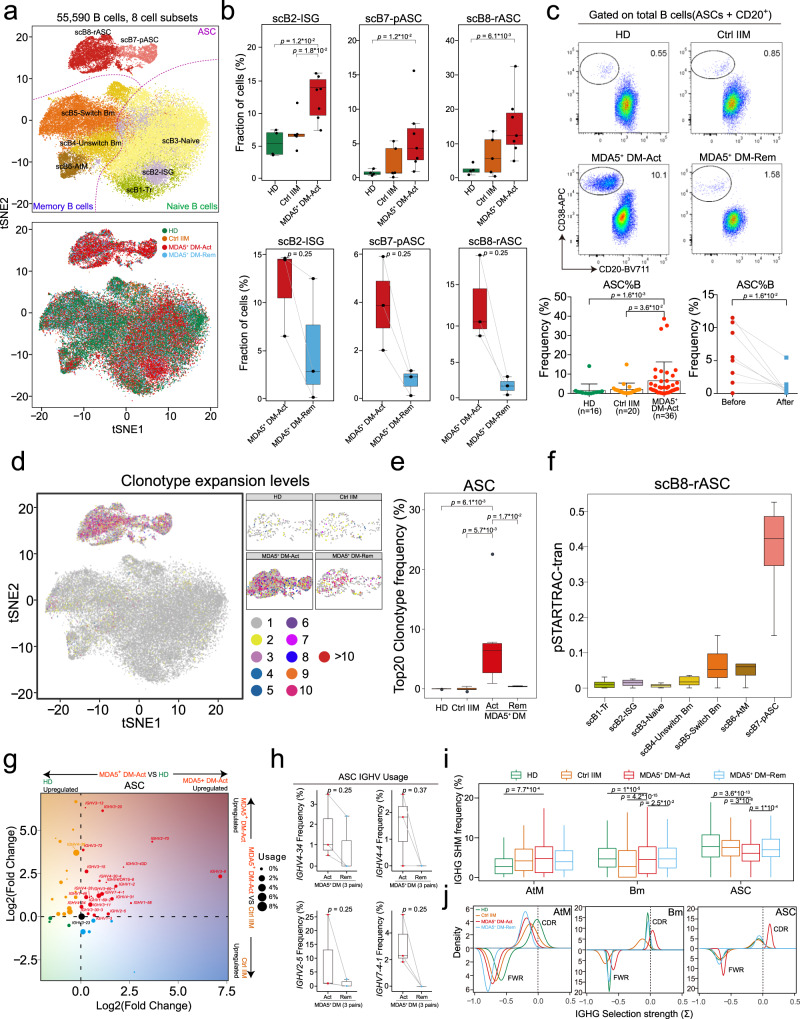
Anti-melanoma differentiation-associated gene 5-positive dermatomyositis (MDA5+ DM) is an autoimmune condition associated with rapidly progressive interstitial lung disease and high mortality. The aetiology and pathogenesis of MDA5+ DM are still largely unknown. Here we describe the immune signatures of MDA5+ DM via single-cell RNA sequencing, flow cytometry and multiplex immunohistochemistry in peripheral B and T cells and in affected lung tissue samples from one patient. We find strong peripheral antibody-secreting cell and CD8+ T cell responses as cellular immune hallmarks, and over-stimulated type I interferon signaling and associated metabolic reprogramming as molecular immune signature in MDA5+ DM. High frequency of circulating ISG15+ CD8+ T cells at baseline predicts poor one-year survival in MDA5+ DM patients. In affected lungs, we find profuse immune cells infiltration, which likely contributes to the pro-fibrotic response via type I interferon production. The importance of type I interferons in MDA5+ DM pathology is further emphasized by our observation in a retrospective cohort of MDA5+ DM patients that combined calcineurin and Janus kinase inhibitor therapy show superior efficacy to calcineurin inhibitor monotherapy. In summary, this study reveals key immune-pathogenic features of MDA5+ DM and provides a potential basis for future tailored therapies.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






Comment in
-
Mapping the immune landscape of MDA5+ dermatomyositis.Nat Rev Rheumatol. 2023 Jan;19(1):3. doi: 10.1038/s41584-022-00879-0. Nat Rev Rheumatol. 2023. PMID: 36400949 No abstract available.
References
-
- Lundberg IE, et al. Idiopathic inflammatory myopathies. Nat. Rev. Dis. Prim. 2021;7:86. - PubMed
-
- Mammen AL, Allenbach Y, Stenzel W, Benveniste O, Group, E.t.W.S. 239th ENMC International Workshop: Classification of dermatomyositis, Amsterdam, the Netherlands, 14-16 December 2018. Neuromuscul. Disord. 2020;30:70–92. - PubMed
-
- Wu W, et al. Interstitial lung disease in anti-MDA5 positive dermatomyositis. Clin. Rev. Allergy Immunol. 2021;60:293–304. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
