

Prediction and evaluation of high-risk patients with primary biliary cholangitis receiving ursodeoxycholic acid therapy: an early criterion
- PMID: 36309918
- PMCID: PMC9895005
- DOI: 10.1007/s12072-022-10431-7
Prediction and evaluation of high-risk patients with primary biliary cholangitis receiving ursodeoxycholic acid therapy: an early criterion
Abstract
Background and aims: Current treatment guidelines recommend ursodeoxycholic acid (UDCA) as the first-line treatment for new-diagnosed primary biliary cholangitis (PBC) patients. However, up to 40% patients are insensitive to UDCA monotherapy, and evaluation of UDCA response at 12 months may result in long period of ineffective treatment. We aimed to develop a new criterion to reliably identify non-response patients much earlier.
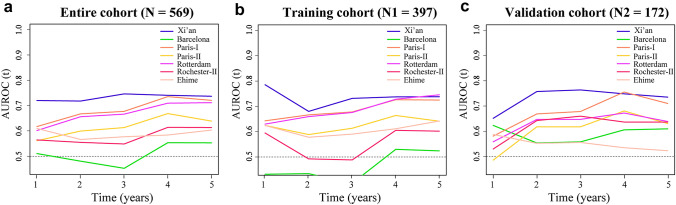
Methods: Five hundred sixty-nine patients with an average of 59 months (Median: 53; IQR:32-79) follow-up periods were randomly divided into either the training (70%) or the validation cohort (30%). The efficiency of different combinations of total bilirubin (TBIL), alkaline phosphatase (ALP), and aspartate aminotransferase (AST) threshold values to predict outcomes was assessed at 1, 3 or 6 month after the initiation of UDCA therapy. The endpoints were defined as adverse outcomes, including liver-related death, liver transplantation and complications of cirrhosis. Adverse outcome-free survival was compared using various published criteria and a proposed new criterion.
Results: A new criterion of evaluating UDCA responses at 1 month was established as: ALP ≤ 2.5 × upper limit of normal (ULN) and AST ≤ 2 × ULN, and TBIL ≤ 1 × ULN (Xi'an criterion). The 5 year adverse outcome-free survival rate of UDCA responders, defined by Xi'an criterion, was 97%, which was significantly higher than that of those non-responders (64%). An accurate distinguishing high-risk patients' capacity of Xi'an criterion was confirmed in both early and late-stage PBC.
Conclusions: Xi'an criterion has a similar or even higher ability to distinguish high-risk PBC patients than other published criteria. Xi'an criterion can facilitate early identification of patients requiring new therapeutic approaches.
Keywords: Adverse outcome; Autoimmune liver disease; Biochemical response; Complication; Early prediction; Primary biliary cholangitis; Prognosis; Retrospective cohort study; Stratified therapy; Therapeutics.
© 2022. The Author(s).
Conflict of interest statement
Chunmei Yang, Guanya Guo, Bo Li, Linhua Zheng, Ruiqing Sun, Xiufang Wang, Juan Deng, Gui Jia, Xia Zhou, Lina Cui, Changcun Guo, Xinmin Zhou, Patrick S. C. Leung, M. Eric Gershwin, Yulong Shang and Ying Han declared that there are no conflicts of interest.
Figures



Similar articles
-
Biochemical response to ursodeoxycholic acid and long-term prognosis in primary biliary cirrhosis.Hepatology. 2008 Sep;48(3):871-7. doi: 10.1002/hep.22428. Hepatology. 2008. PMID: 18752324
-
Early primary biliary cirrhosis: biochemical response to treatment and prediction of long-term outcome.J Hepatol. 2011 Dec;55(6):1361-7. doi: 10.1016/j.jhep.2011.02.031. Epub 2011 Apr 13. J Hepatol. 2011. PMID: 21703194
-
Improved prognosis of patients with primary biliary cirrhosis that have a biochemical response to ursodeoxycholic acid.Gastroenterology. 2009 Apr;136(4):1281-7. doi: 10.1053/j.gastro.2009.01.003. Epub 2009 Jan 14. Gastroenterology. 2009. PMID: 19208346
-
Obeticholic acid for the treatment of primary biliary cholangitis.Expert Opin Pharmacother. 2016 Sep;17(13):1809-15. doi: 10.1080/14656566.2016.1218471. Epub 2016 Aug 9. Expert Opin Pharmacother. 2016. PMID: 27468093 Review.
-
Treatment response to ursodeoxycholic acid in primary biliary cholangitis: A systematic review and meta-analysis.Dig Liver Dis. 2023 Oct;55(10):1318-1327. doi: 10.1016/j.dld.2022.12.010. Epub 2022 Dec 31. Dig Liver Dis. 2023. PMID: 36593158
Cited by
-
The treatment of primary biliary cholangitis: from shadow to light.Therap Adv Gastroenterol. 2024 Jul 29;17:17562848241265782. doi: 10.1177/17562848241265782. eCollection 2024. Therap Adv Gastroenterol. 2024. PMID: 39081664 Free PMC article. Review.
-
Prognostic significance of liver stiffness in patients with primary biliary cholangitis: validation of Baveno VII criteria.Hepatol Int. 2024 Feb;18(1):206-215. doi: 10.1007/s12072-023-10587-w. Epub 2023 Sep 19. Hepatol Int. 2024. PMID: 37725332 Free PMC article.
-
Early assessment of treatment response in primary biliary cholangitis: key to timely management.BMC Gastroenterol. 2025 Aug 9;25(1):571. doi: 10.1186/s12876-025-04138-w. BMC Gastroenterol. 2025. PMID: 40783513 Free PMC article.
-
MGAT5/TMEM163 variant is associated with prognosis in ursodeoxycholic acid-treated patients with primary biliary cholangitis.J Gastroenterol. 2024 Jan;59(1):66-74. doi: 10.1007/s00535-023-02045-z. Epub 2023 Oct 16. J Gastroenterol. 2024. PMID: 37845416
-
The External Validation of GLOBE and UK-PBC Risk Scores for Predicting Ursodeoxycholic Acid Treatment Response in a Large U.S. Cohort of Primary Biliary Cholangitis Patients.J Clin Med. 2024 Aug 1;13(15):4497. doi: 10.3390/jcm13154497. J Clin Med. 2024. PMID: 39124763 Free PMC article.
