

Pathophysiology of polycystic ovary syndrome revisited: Current understanding and perspectives regarding future research
- PMID: 36310656
- PMCID: PMC9601867
- DOI: 10.1002/rmb2.12487
Pathophysiology of polycystic ovary syndrome revisited: Current understanding and perspectives regarding future research
Abstract
Background: Polycystic ovary syndrome (PCOS) is the most common endocrine disorder among reproductive-age women and has lifelong effects on health.
Methods: In this review, I discuss the pathophysiology of PCOS. First, I summarize our current understanding of the etiology and pathology of PCOS, then, discuss details of two representative environmental factors involved in the pathogenesis of PCOS. Finally, I present perspectives regarding the directions of future research.
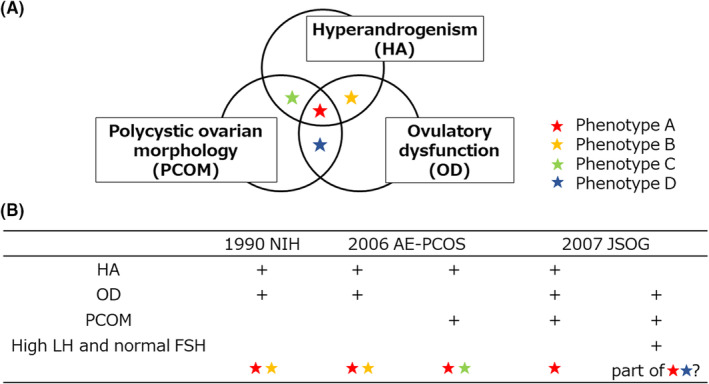
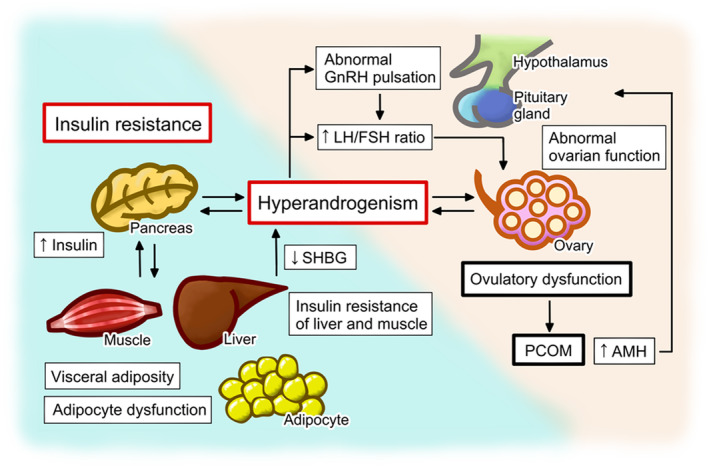
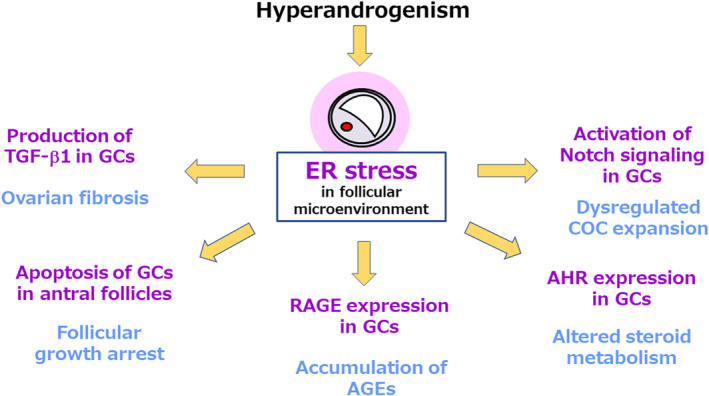
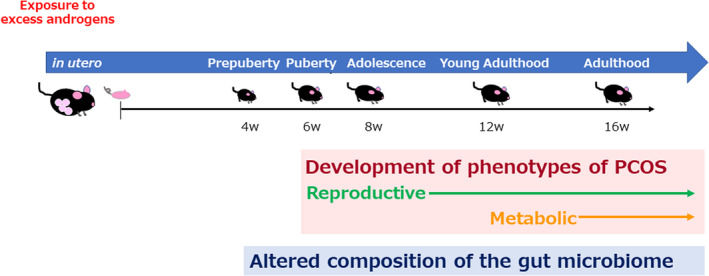
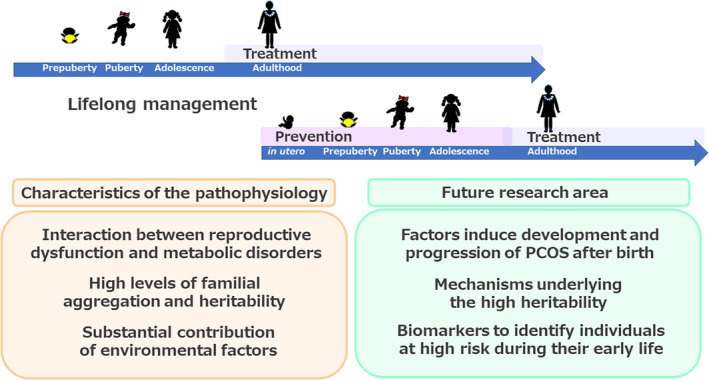
Main findings: The pathophysiology of PCOS is heterogeneous and shaped by the interaction of reproductive dysfunction and metabolic disorders. Hyperandrogenism and insulin resistance exacerbate one another during the development of PCOS, which is also affected by dysfunction of the hypothalamus-pituitary-ovarian axis. PCOS is a highly heritable disorder, and exposure to certain environmental factors causes individuals with predisposing genetic factors to develop PCOS. The environmental factors that drive the development of PCOS pathophysiology make a larger contribution than the genetic factors, and may include the intrauterine environment during the prenatal period, the follicular microenvironment, and lifestyle after birth.
Conclusion: On the basis of this current understanding, three areas are proposed to be subjects for future research, with the ultimate goals of developing therapeutic and preventive strategies and providing appropriate lifelong management, including preconception care.
Keywords: delayed effects of prenatal exposure; endoplasmic reticulum stress (ER stress); follicular microenvironment; gastrointestinal microbiome; polycystic ovary syndrome (PCOS).
© 2022 The Author. Reproductive Medicine and Biology published by John Wiley & Sons Australia, Ltd on behalf of Japan Society for Reproductive Medicine.
Conflict of interest statement
Miyuki Harada declares that she has no conflict of interest.
Figures
References
-
- Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta‐analysis. Hum Reprod. 2016;31:2841–55. - PubMed
-
- Rotterdam ESHRE/ASRM‐Sponsored PCOS Consensus Workshop Group . Revised 2003 consensus on diagnostic criteria and long‐term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19:41–7. - PubMed
-
- International PCOS Network in Collaboration with Funding Partner and Collaborating Partners. International evidence‐based guideline for the assessment and management of polycystic ovary syndrome 2018. https://www.monash.edu/__data/assets/pdf_file/0004/1412644/PCOS_Evidence.... 2018. Accessed 17 Jun 2022.
-
- Azziz R, Carmina E, Dewailly D, Diamanti‐Kandarakis E, Escobar‐Morreale HF, Futterweit W, et al. Positions statement: criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an androgen excess society guideline. J Clin Endocrinol Metab. 2006;91:4237–45. - PubMed
LinkOut - more resources
Full Text Sources