

doi: 10.1016/j.eats.2022.05.015.
eCollection 2022 Oct.
All-arthroscopic Knee Patellofemoral Ligament Repair
Affiliations
- PMID: 36311312
- PMCID: PMC9596889
- DOI: 10.1016/j.eats.2022.05.015
Item in Clipboard
All-arthroscopic Knee Patellofemoral Ligament Repair
Arthrosc Tech.
.
Abstract
Patellar dislocations are common injuries in the pediatric and adolescent population, with an estimated mean incidence of 42/100,000 person-years. The medial patellofemoral ligament is the most important structure preventing lateral patellar translation, whereas its patellar attachment is frequently damaged after patellar dislocations. This technical note presents an all-arthroscopic medial patellofemoral ligament repair technique suggested after a first episode of patellar dislocation.
© 2022 The Authors.
Figures
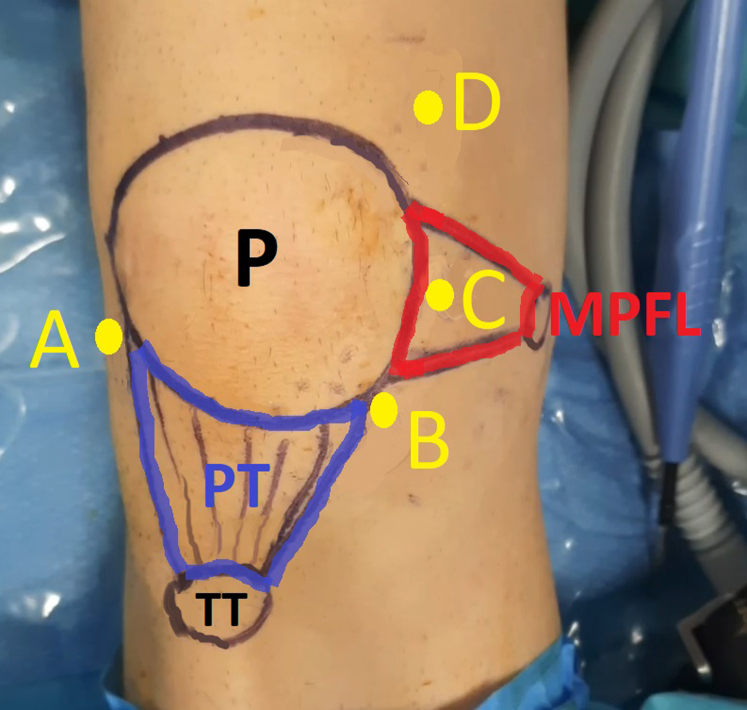
Identification of the anatomic structures before surgery is essential. Surgery is performed using 4 working portals: lateral portal (portal A) for viewing, medial portal (portal B) for suture management, central-medial portal (portal C) for anchor placement and knot tying, and superior-medial portal (portal D) for suture management. A right knee is shown. (MPFL, medial patellofemoral ligament; P, patella; PT, patellar tendon; TT, tibial tubercle.)
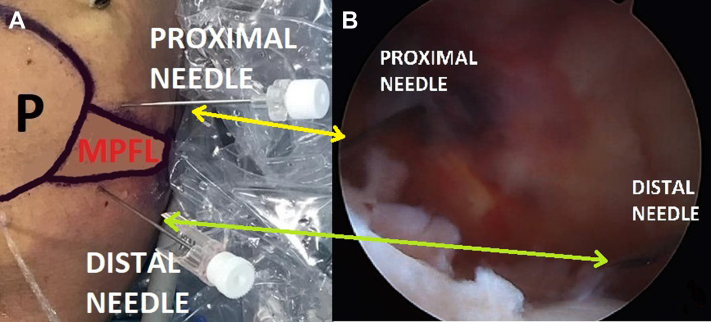
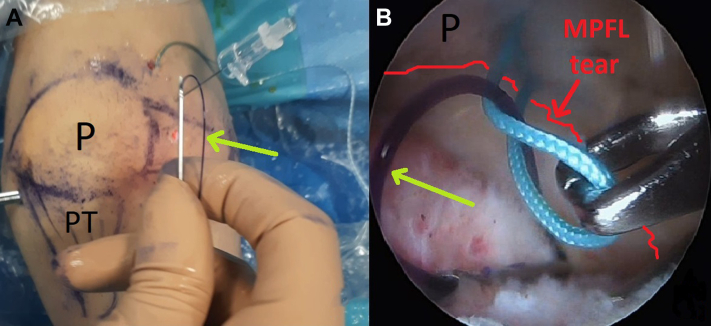
(A) Right knee. (B) Intra-articular arthroscopic visualization of right knee from portal A (lateral portal) with knee kept in full extension. Placement of spinal needles on the proximal border (yellow arrow) and distal border (green arrow) of the medial patellofemoral ligament (MPFL) previously outlined on the skin (A) helps in understanding the course of the ligament from the intra-articular side (B). (P, patella.)
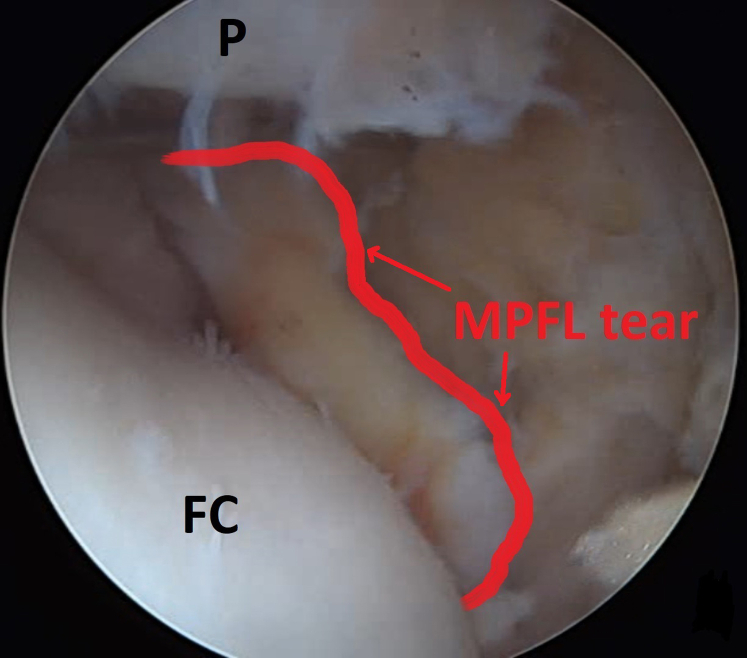
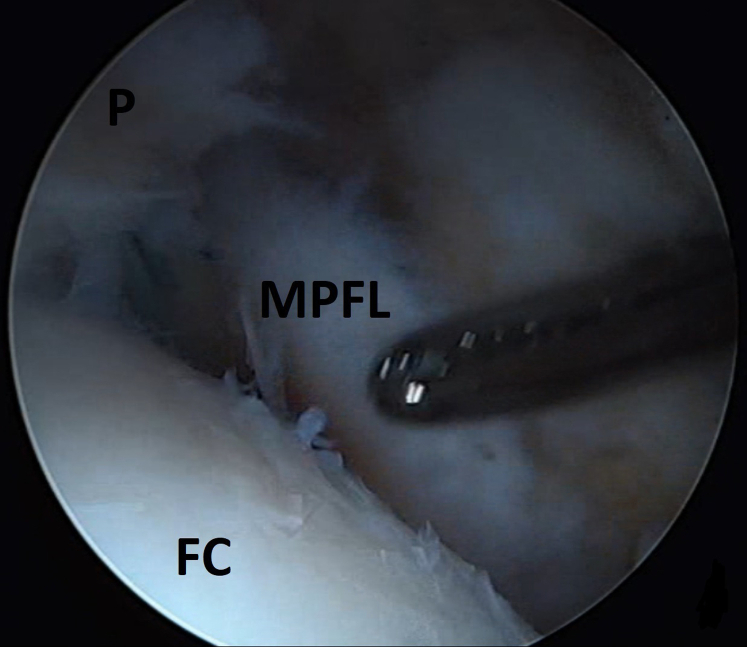
Intra-articular arthroscopic visualization of right knee from portal A (lateral portal) with knee kept in full extension. After debridement with an arthroscopic shaver through portals B (medial portal) and D (superior-medial portal), the medial patellofemoral ligament (MPFL) tear (red arrows) is exposed. (FC, femoral condyle; P, patella.)
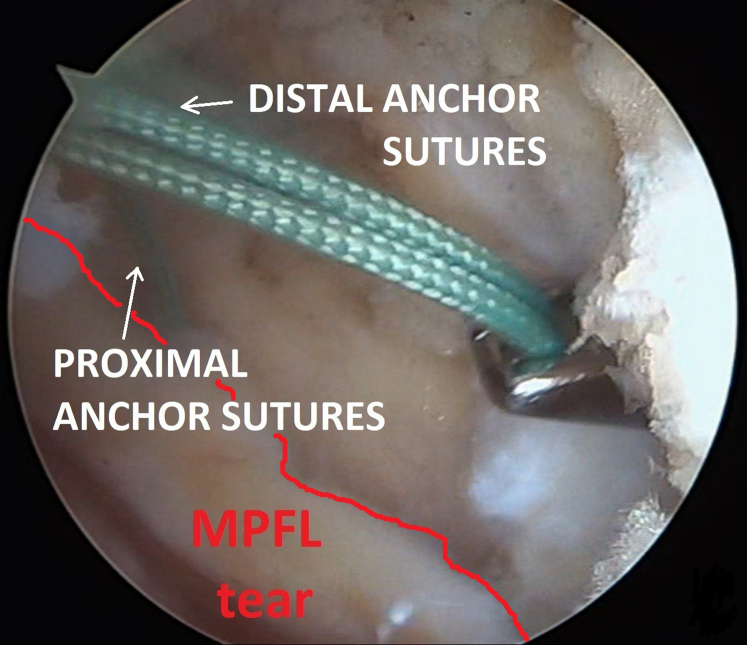
Intra-articular arthroscopic visualization of right knee from portal A (lateral portal) with knee kept in full extension. After placement of 1 proximally and 1 distally placed Iconix 2.3-mm all-suture anchor implanted through portal C (central portal), the proximal anchor sutures are retrieved through portal D and the distal anchor sutures are retrieved through portal B (white arrows). (MPFL, medial patellofemoral ligament.)
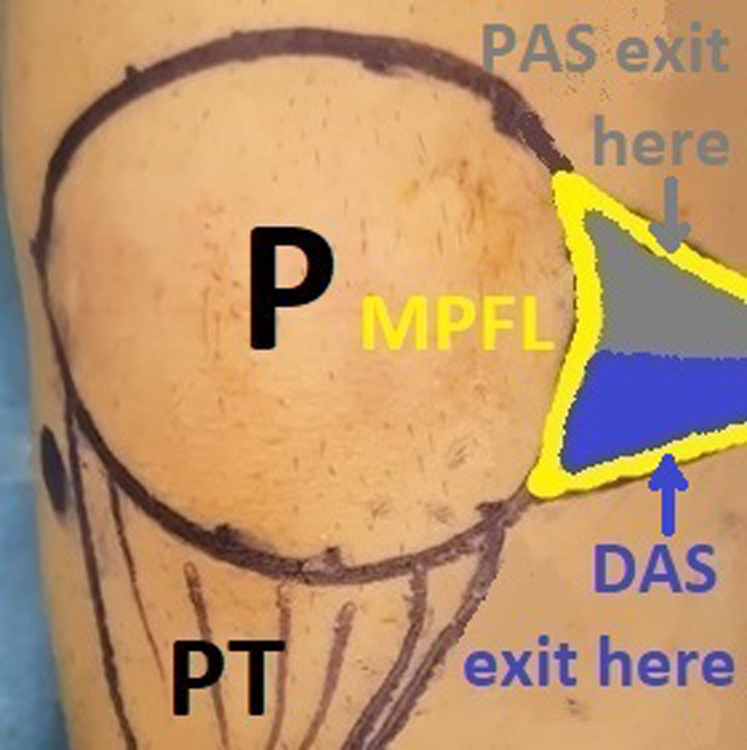
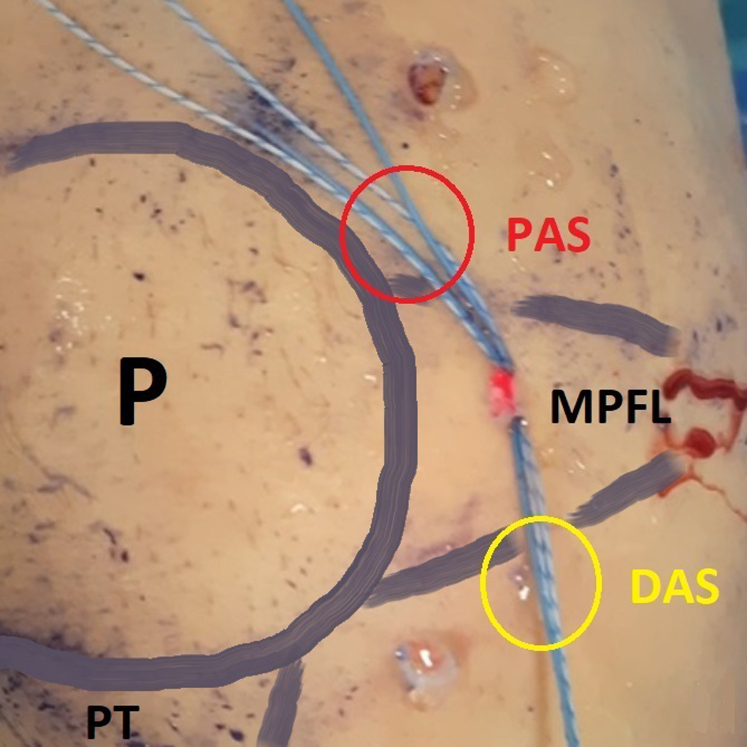
The goal of the surgical procedure is to shuttle the proximal anchor sutures (PAS) through the proximal half of the medial patellofemoral ligament (MPFL) (gray arrow) and the distal anchor sutures (DAS) through the distal half of the MPFL (blue arrow). A right knee is shown. (P, patella; PT, patellar tendon.)
(A) Right knee. (B) Intra-articular arthroscopic visualization of right knee from portal A (lateral portal) with knee kept in full extension. An 18-gauge spinal needle is loaded with a No. 1 polydioxanone suture acting as a loop (A) (yellow arrow) and introduced percutaneously piercing the medial patellofemoral ligament (MPFL) tissue at the desired location starting from the proximal half of the MPFL tissue (B) (yellow arrow). The green suture of the proximal anchor is retrieved through the loop, followed by retrieval of the spinal needle, thus shuttling the green suture through the MPFL tissue. (DAS, distal anchor sutures; FC, femoral condyle; P, patella; PAS, proximal anchor sutures; PT, patellar tendon; TT, tibial tubercle.)
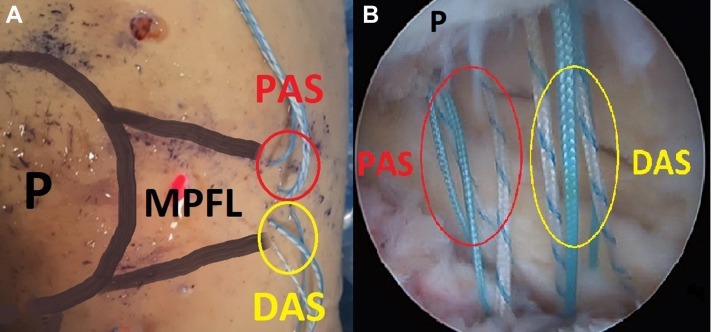
(A) Right knee. (B) Intra-articular arthroscopic visualization of right knee from portal A (lateral portal) with knee kept in full extension. The proximal anchor sutures (PAS) (red ovals) and distal anchor sutures (DAS) (yellow ovals) have been shuttled through the medial patellofemoral ligament (MPFL) tissue. (P, patella.)
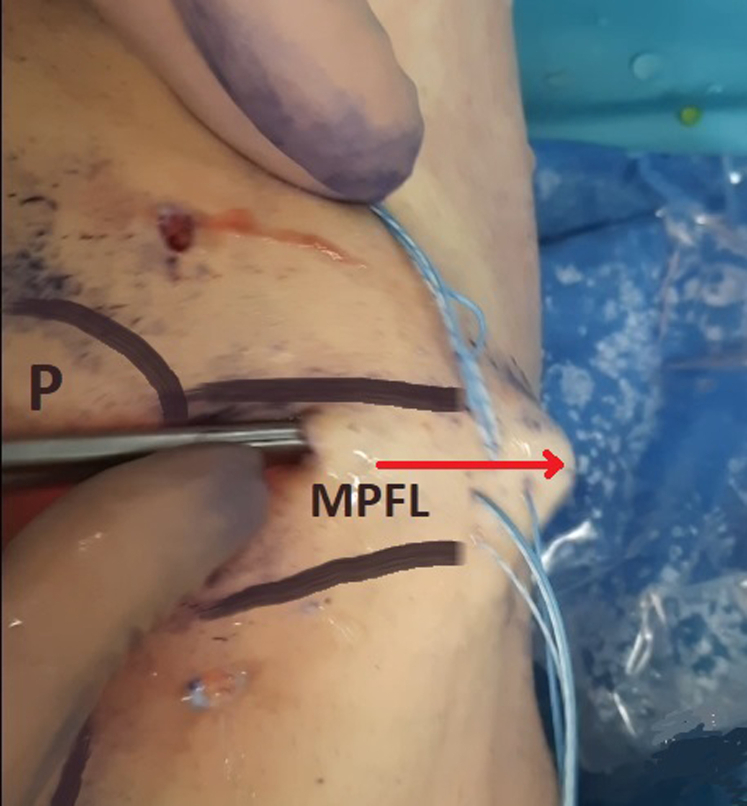
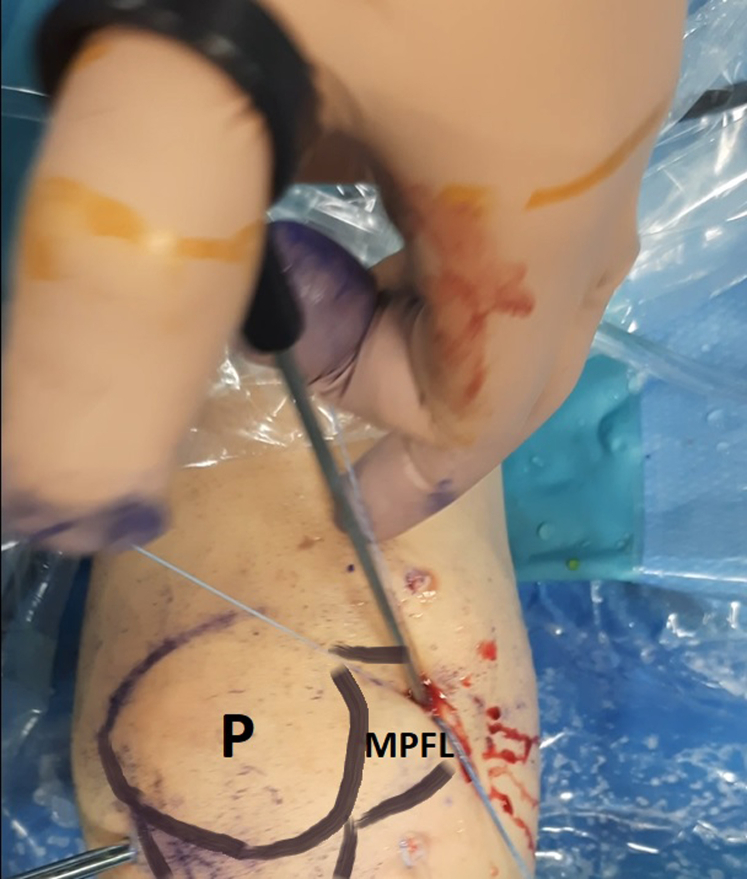
A Pean forceps is introduced through portal C (central-medial portal) and bluntly divides the subcutaneous plane, moving toward the direction of the medial femoral condyle (red arrow). A right knee is shown. (MPFL, medial patellofemoral ligament; P, patella.)
The anchor sutures have been retrieved through portal C (central-medial portal) using a suture retriever introduced in the subcutaneous plane. Subsequently, the proximal anchor sutures (PAS) (red oval) and distal anchor sutures (DAS) (yellow oval) are divided. A right knee is shown. (MPFL, medial patellofemoral ligament; P, patella; PT, patellar tendon.)
Anchor sutures are sequentially tied in a proximal-to-distal direction using standard arthroscopic sliding knots. A right knee is shown. (MPFL, medial patellofemoral ligament; P, patella.)
Intra-articular arthroscopic visualization of right knee from portal A (lateral portal) with knee kept in full extension. The medial patellofemoral ligament (MPFL) has been reinserted on the patella (P) and is probed for adequate tension. (FC, femoral condyle.)
References
-
- Gravesen K.S., Kallemose T., Blønd L., Troelsen A., Barfod K.W. High incidence of acute and recurrent patellar dislocations: A retrospective nationwide epidemiological study involving 24.154 primary dislocations. Knee Surg Sports Traumatol Arthrosc. 2018;26:1204–1209. - PubMed
-
- Amis A.A., Firer P., Mountney J., Senavongse W., Thomas N.P. Anatomy and biomechanics of the medial patellofemoral ligament. Knee. 2003;10:215–220. - PubMed
-
- Kepler C.K., Bogner E.A., Hammoud S., Malcolmson G., Potter H.G., Green D.W. Zone of injury of the medial patellofemoral ligament after acute patellar dislocation in children and adolescents. Am J Sports Med. 2011;39:1444–1449. - PubMed
LinkOut - more resources
Full Text Sources
