

Anchor Arthropathy Caused by Cartilage Penetration: An Approach to Revision Hip Arthroscopy With Removal of Problematic Anchors
- PMID: 36311313
- PMCID: PMC9596390
- DOI: 10.1016/j.eats.2022.06.003
Anchor Arthropathy Caused by Cartilage Penetration: An Approach to Revision Hip Arthroscopy With Removal of Problematic Anchors
Abstract
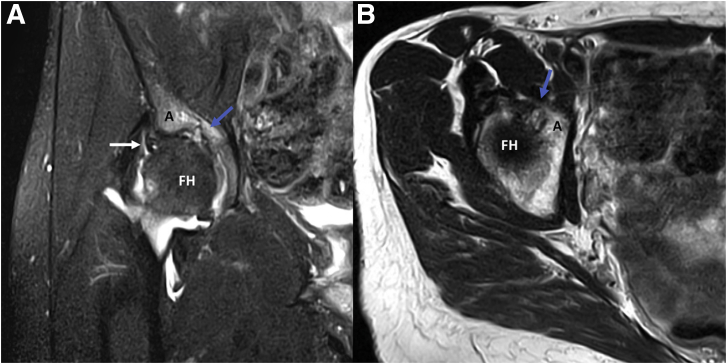
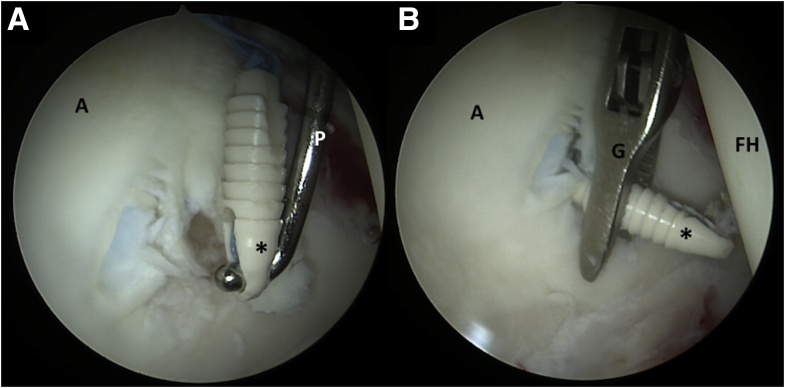
Hip arthroscopy has been proven to effectively treat labral tears in the setting of femoroacetabular impingement. Anchors used for this treatment have constantly evolved and improved to ensure safety and minimal invasion. However, acetabular drilling and anchor placement are technically challenging due to the concavity of the acetabular articular surface, limited angles for anchor insertion, and finite bone availability in the anterior and posterior column. Inadequate technique can result in protruding anchors, which may lead to full-thickness articular cartilage damage, manifesting in pain, mechanical symptoms, and impaired function. This Technical Note demonstrates arthroscopic removal of protruding anchors and management of the iatrogenic grade IV cartilage damage. In this description, the technical pearls and pitfalls of acetabular anchor placement to treat labral pathology are presented along with the aforementioned technique.
© 2022 The Authors.
Figures
References
-
- Ferguson S.J., Bryant J.T., Ganz R., Ito K. The influence of the acetabular labrum on hip joint cartilage consolidation: a poroelastic finite element model. J Biomech. 2000;33:953–960. - PubMed
-
- Nepple J.J., Philippon M.J., Campbell K.J., et al. The hip fluid seal—Part II: The effect of an acetabular labral tear, repair, resection, and reconstruction on hip stability to distraction. Knee Surg Sports Traumatol Arthrosc. 2014;22:730–736. - PubMed
-
- Maldonado D.R., Kyin C., Chen S.L., et al. In search of labral restoration function with hip arthroscopy: outcomes of hip labral reconstruction versus labral repair: A systematic review. HIP Int. 2021;31:704–713. - PubMed
-
- Kyin C., Maldonado D.R., Go C.C., Shapira J., Lall A.C., Domb B.G. Mid- to long-term outcomes of hip arthroscopy: A systematic review. Arthroscopy. 2021;37:1011–1025. - PubMed
-
- Schüttler K.F., Schramm R., El-Zayat B.F., Schofer M.D., Efe T., Heyse T.J. The effect of surgeon’s learning curve: Complications and outcome after hip arthroscopy. Arch Orthop Trauma Surg. 2018;138:1415–1421. - PubMed
LinkOut - more resources
Full Text Sources
