

The hidden financial catastrophe of chronic kidney disease under universal coverage and Thai "Peritoneal Dialysis First Policy"
- PMID: 36311589
- PMCID: PMC9606783
- DOI: 10.3389/fpubh.2022.965808
The hidden financial catastrophe of chronic kidney disease under universal coverage and Thai "Peritoneal Dialysis First Policy"
Abstract
Objective: Universal health coverage can decrease the magnitude of the individual patient's financial burden of chronic kidney disease (CKD), but the residual financial hardship from the patients' perspective has not been well-studied in low and middle-income countries (LMICs). This study aimed to evaluate the residual financial burden in patients with CKD stage 3 to dialysis in the "PD First Policy" under Universal Coverage Scheme (UCS) in Thailand.
Methods: This multicenter nationwide cross-sectional study in Thailand enrolled 1,224 patients with pre-dialysis CKD, hemodialysis (HD), and peritoneal dialysis (PD) covered by UCS and other health schemes for employees and civil servants. We interviewed patients to estimate the proportion with catastrophic health expenditure (CHE) and medical impoverishment. The risk factors associated with CHE were analyzed by multivariable logistic regression.
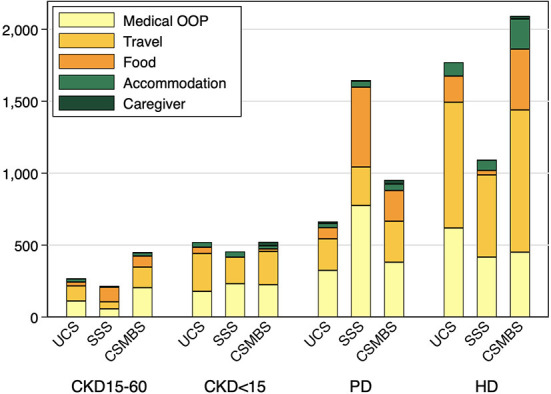
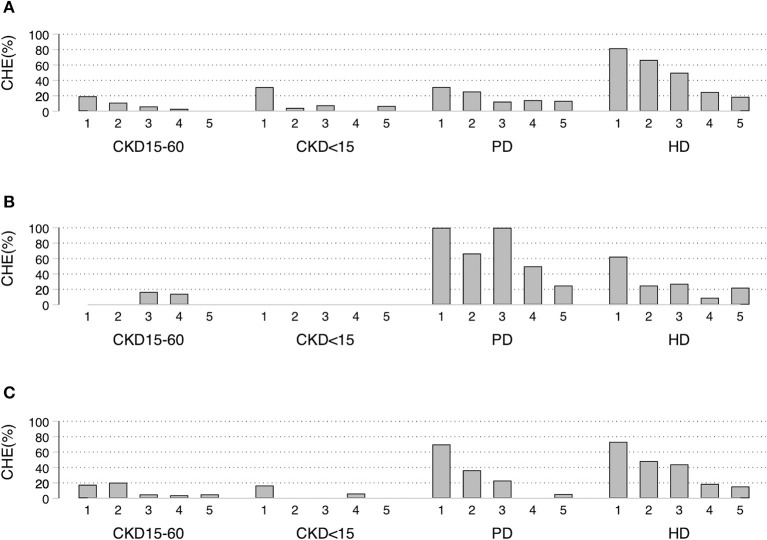
Results: Under UCS, the total out-of-pocket expenditure in HD was over two times higher than PD and nearly six times higher than CKD stages 3-4. HD suffered significantly more CHE and medical impoverishment than PD and pre-dialysis CKD [CHE: 8.5, 9.3, 19.5, 50.0% (p < 0.001) and medical impoverishment: 8.0, 3.1, 11.5, 31.6% (p < 0.001) for CKD Stages 3-4, Stage 5, PD, and HD, respectively]. In the poorest quintile of UCS, medical impoverishment was present in all HD and two-thirds of PD patients. Travel cost was the main driver of CHE in HD. In UCS, the adjusted risk of CHE increased in PD and HD (OR: 3.5 and 16.3, respectively) compared to CKD stage 3.
Conclusions: Despite universal coverage, the residual financial burden remained high in patients with kidney failure. CHE was considerably lower in PD than HD, although the rates remained alarmingly high in the poor. The "PD First' program" could serve as a model for other LMICs. However, strategies to minimize financial distress should be further developed, especially for the poor.
Keywords: Asia; catastrophic health expenditure; economic; impoverishment; kidney failure; universal health insurance.
Copyright © 2022 Sangthawan, Klyprayong, Geater, Tanvejsilp, Anutrakulchai, Boongird, Gojaseni, Kuhiran, Lorvinitnun, Noppakun, Parapiboon, Sirilak, Tankee, Taruangsri, Sangsupawanich, Sritara, Chaiyakunapruk and Kitiyakara.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Quality of Life in Patients with CKD With Catastrophic Health Care Expenditures: A National Study From Thailand.Kidney Med. 2025 Feb 27;7(5):100987. doi: 10.1016/j.xkme.2025.100987. eCollection 2025 May. Kidney Med. 2025. PMID: 40256210 Free PMC article.
-
Mortality and treatment costs of hospitalized chronic kidney disease patients between the three major health insurance schemes in Thailand.BMC Health Serv Res. 2016 Sep 29;16(1):528. doi: 10.1186/s12913-016-1792-9. BMC Health Serv Res. 2016. PMID: 27686066 Free PMC article.
-
Financial toxicity of cancer treatment in India: towards closing the cancer care gap.Front Public Health. 2023 Jun 19;11:1065737. doi: 10.3389/fpubh.2023.1065737. eCollection 2023. Front Public Health. 2023. PMID: 37404274 Free PMC article.
-
PD First Policy: Thailand's Response to the Challenge of Meeting the Needs of Patients With End-Stage Renal Disease.Semin Nephrol. 2017 May;37(3):287-295. doi: 10.1016/j.semnephrol.2017.02.008. Semin Nephrol. 2017. PMID: 28532557 Review.
-
Peritoneal Dialysis in Asia.Kidney Dis (Basel). 2015 Dec;1(3):147-56. doi: 10.1159/000439193. Epub 2015 Sep 11. Kidney Dis (Basel). 2015. PMID: 27536675 Free PMC article. Review.
Cited by
-
Capacity for the management of kidney failure in the International Society of Nephrology Eastern and Central Europe region: report from the 2023 ISN Global Kidney Health Atlas (ISN-GKHA).Kidney Int Suppl (2011). 2024 Apr;13(1):29-42. doi: 10.1016/j.kisu.2024.01.006. Epub 2024 Apr 8. Kidney Int Suppl (2011). 2024. PMID: 38618499 Free PMC article. Review.
-
Landscape of kidney replacement therapy provision in low- and lower-middle income countries: A multinational study from the ISN-GKHA.PLOS Glob Public Health. 2024 Dec 2;4(12):e0003979. doi: 10.1371/journal.pgph.0003979. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39621612 Free PMC article.
-
Financial Toxicity and Kidney Disease in Children and Adults: A Scoping Review.Int J Nephrol Renovasc Dis. 2025 Jan 21;18:13-25. doi: 10.2147/IJNRD.S485111. eCollection 2025. Int J Nephrol Renovasc Dis. 2025. PMID: 39872022 Free PMC article. Review.
-
Financial Toxicity in Renal Patients (FINTORE) Study: A Cross-Sectional Italian Study on Financial Burden in Kidney Disease-A Project Protocol.Methods Protoc. 2024 Apr 14;7(2):34. doi: 10.3390/mps7020034. Methods Protoc. 2024. PMID: 38668141 Free PMC article.
-
Quality of Life in Patients with CKD With Catastrophic Health Care Expenditures: A National Study From Thailand.Kidney Med. 2025 Feb 27;7(5):100987. doi: 10.1016/j.xkme.2025.100987. eCollection 2025 May. Kidney Med. 2025. PMID: 40256210 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical