

Postoperative serum myoglobin as a predictor of early allograft dysfunction after liver transplantation
- PMID: 36311930
- PMCID: PMC9597078
- DOI: 10.3389/fsurg.2022.1026586
Postoperative serum myoglobin as a predictor of early allograft dysfunction after liver transplantation
Abstract
Background: Early allograft dysfunction (EAD) is a common postliver transplant complication that has been associated with graft failure and risk for poor prognosis. There are many risk factors for the incidence of EAD after liver transplantation (LT). This study investigated whether elevated postoperative myoglobin (Mb) increases the incidence of EAD in liver transplanted recipients.
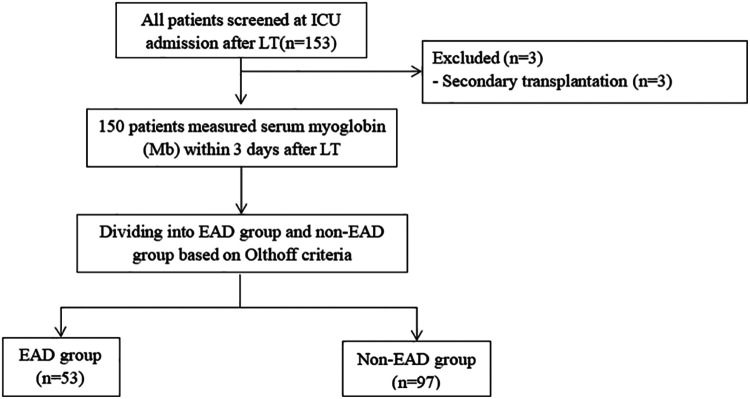
Methods: A total of 150 adult recipients who measured Mb within 3 days after liver transplantation between June 2019 and June 2021 were evaluated. Then, all patients were divided into two groups: the EAD group and the non-EAD group. Univariate and multivariate logistic regression analyses were performed, and receiver operating characteristic curves (ROCs) were constructed.
Results: The incidence of EAD was 53 out of 150 patients (35.3%) in our study. Based on the multivariate logistic analysis, the risk of EAD increased with elevated postoperative Mb (OR = 1.001, 95% CI 1.000-1.001, P = 0.002). The Mb AUC was 0.657, and it was 0.695 when combined with PCT. When the subgroup analysis was conducted, the AUC of serum Mb prediction was better in patients whose preoperative model for end-stage liver disease score ≤ 15 or operative time ≥ 10 h (AUC = 0.751, 0.758, respectively, or 0.760, 0.800 when combined with PCT).
Conclusion: Elevated Mb significantly increased the risk of postoperative EAD, suggesting that postoperative Mb may be a novel predictor of EAD after liver transplantation.The study was registered in the Chinese Clinical Trial Registry (Registration number: ChiCTR2100044257, URL: http://www.chictr.org.cn).
Keywords: complication; early allograft dysfunction; liver transplantation; myoglobin; predictor.
© 2022 Zhang, Han, Ke, Gao, Shi, Zhao, You, Jia, Ding, Zheng, Li and Huang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Brea-Gómez E, Villar-Quintana R, Plata-lllescas C, Zambudio-Carroll N, Lopez-Garrido MA, Nogueras-Lopez F, et al. Analysis of the predictive ability for graft loss and mortality of two criteria for early allograft dysfunction after liver transplantation. Transplant Proc. (2018) 50:605–9. 10.1016/j.transproceed.2017.11.057 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous