

Association between minimally invasive surgery and late seizures in patients with intracerebral hemorrhage: A propensity score matching study
- PMID: 36311938
- PMCID: PMC9606625
- DOI: 10.3389/fsurg.2022.949804
Association between minimally invasive surgery and late seizures in patients with intracerebral hemorrhage: A propensity score matching study
Abstract
Purpose: The association between minimally invasive surgery (MIS) for hematoma evacuation and late seizures after intracerebral hemorrhage (ICH) remains uncertain. We aimed to investigate whether MIS increases the risk of late seizures after ICH and identify the risk factors for late seizures in this patient subgroup.
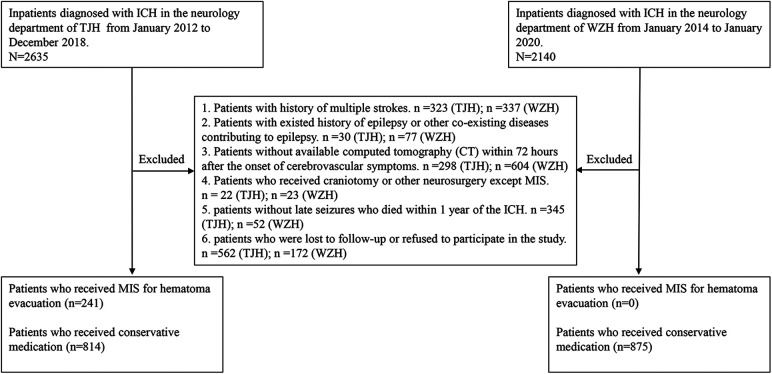
Methods: We retrospectively included consecutive inpatients diagnosed with ICH at two tertiary hospitals in China. The subjects were divided into the MIS group (ICH patients who received MIS including hematoma aspiration and thrombolysis) and conservative treatment group (ICH patients who received conservative medication). Propensity score matching was performed to balance possible risk factors for late seizures between the MIS and conservative treatment groups. Before and after matching, between-group comparisons of the incidence of late seizures were performed between the MIS and conservative treatment groups. Univariate and multivariate logistic regression analyses were used to identify independent risk factors for late seizures in MIS-treated patients.
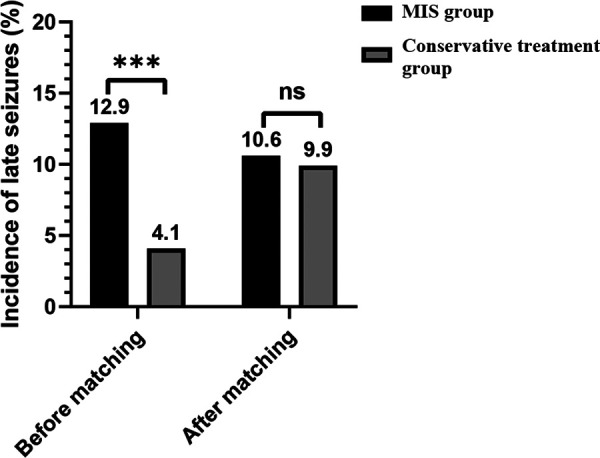
Results: A total of 241 and 1,689 patients were eligible for the MIS and conservative treatment groups, respectively. After matching, 161 ICH patients from the MIS group were successfully matched with 161 ICH patients from the conservative treatment group (1:1). Significant differences (p < 0.001) were found between the MIS group (31/241, 12.9%) and conservative treatment group (69/1689, 4.1%) in the incidence of late seizures before matching. However, after matching, no significant differences (p = 0.854) were found between the MIS group (17/161, 10.6%) and conservative treatment group (16/161, 9.9%). Multivariate logistic regression analysis revealed that cortical involvement (OR = 2.547; 95% CI = 1.137-5.705; p value = 0.023) and higher National Institutes of Health Stroke Scale (NIHSS) scores (OR = 1.050; 95% CI = 1.008-1.094; p value = 0.019) were independent risk factors for late seizures.
Conclusion: Our study revealed that receiving MIS did not increase the incidence of late seizures after ICH. Additionally, cortical involvement and NIHSS scores were independent risk factors for late seizures in MIS-treated patients.
Keywords: intracerebral hemorrhage; minimally invasive surgery; propensity score matching; risk factor; seizures.
© 2022 Lin, Lin, Li, Ye, Wang, Zhang, Chen, Wang, Huang and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Bedside Catheter Hematoma Evacuation in Vitamin K Antagonist-Related Intracerebral Hemorrhage: A Safe and Feasible Approach.Front Neurol. 2020 Aug 14;11:807. doi: 10.3389/fneur.2020.00807. eCollection 2020. Front Neurol. 2020. PMID: 32922349 Free PMC article.
-
Outcomes Following Minimally Invasive Surgery for Intracerebral Hemorrhage in the AHA Get With The Guidelines-Stroke Registry.Stroke. 2025 Jun;56(6):1441-1450. doi: 10.1161/STROKEAHA.124.048650. Epub 2025 Apr 3. Stroke. 2025. PMID: 40177744
-
Minimally invasive endoscopic hematoma evacuation vs best medical management for spontaneous basal-ganglia intracerebral hemorrhage.J Neurointerv Surg. 2019 Jun;11(6):579-583. doi: 10.1136/neurintsurg-2018-014447. Epub 2019 Jan 7. J Neurointerv Surg. 2019. PMID: 30617144
-
Minimally Invasive Intracerebral Hemorrhage Evacuation Techniques: A Review.Diagnostics (Basel). 2021 Mar 23;11(3):576. doi: 10.3390/diagnostics11030576. Diagnostics (Basel). 2021. PMID: 33806790 Free PMC article. Review.
-
Minimally invasive surgery for intracerebral hemorrhage.Curr Opin Crit Care. 2020 Apr;26(2):129-136. doi: 10.1097/MCC.0000000000000695. Curr Opin Crit Care. 2020. PMID: 32004194 Review.
References
-
- Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the global burden of disease study 2010. Lancet Glob Health. (2013) 1(5):e259–81. 10.1016/S2214-109X(13)70089-5 - DOI - PMC - PubMed
-
- Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the international surgical trial in intracerebral haemorrhage (STICH): a randomised trial. Lancet. (2005) 365(9457):387–97. 10.1016/S0140-6736(05)70233-6 - DOI - PubMed
LinkOut - more resources
Full Text Sources