

Artificial intelligence-assisted remote detection of ST-elevation myocardial infarction using a mini-12-lead electrocardiogram device in prehospital ambulance care
- PMID: 36312246
- PMCID: PMC9614054
- DOI: 10.3389/fcvm.2022.1001982
Artificial intelligence-assisted remote detection of ST-elevation myocardial infarction using a mini-12-lead electrocardiogram device in prehospital ambulance care
Erratum in
-
Corrigendum: Artificial intelligence-assisted remote detection of ST-elevation myocardial infarction using a mini-12-lead electrocardiogram device in prehospital ambulance care.Front Cardiovasc Med. 2022 Dec 9;9:1078223. doi: 10.3389/fcvm.2022.1078223. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36568545 Free PMC article.
Abstract
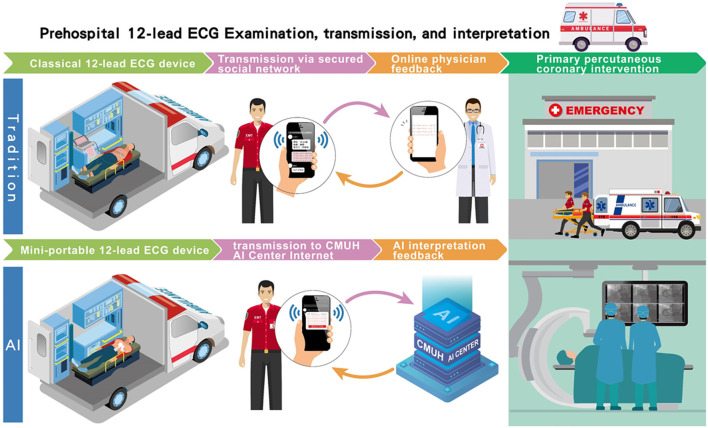
Objective: To implement an all-day online artificial intelligence (AI)-assisted detection of ST-elevation myocardial infarction (STEMI) by prehospital 12-lead electrocardiograms (ECGs) to facilitate patient triage for timely reperfusion therapy.
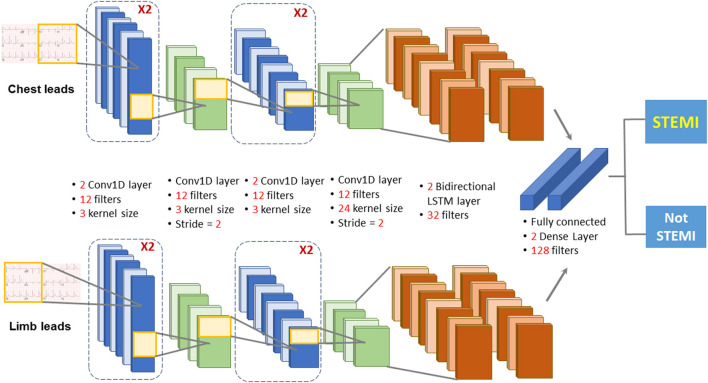
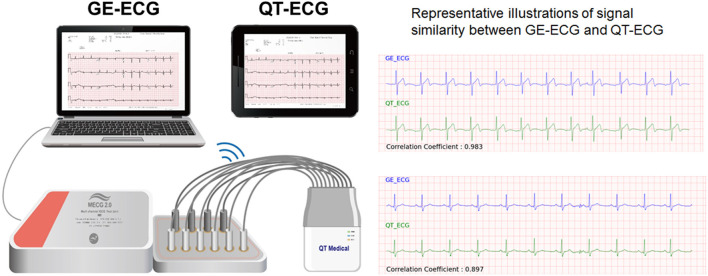
Methods: The proposed AI model combines a convolutional neural network and long short-term memory (CNN-LSTM) to predict STEMI on prehospital 12-lead ECGs obtained from mini-12-lead ECG devices equipped in ambulance vehicles in Central Taiwan. Emergency medical technicians (EMTs) from the 14 AI-implemented fire stations performed the on-site 12-lead ECG examinations using the mini portable device. The 12-lead ECG signals were transmitted to the AI center of China Medical University Hospital to classify the recordings as "STEMI" or "Not STEMI". In 11 non-AI fire stations, the ECG data were transmitted to a secure network and read by available on-line emergency physicians. The response time was defined as the time interval between the ECG transmission and ECG interpretation feedback.
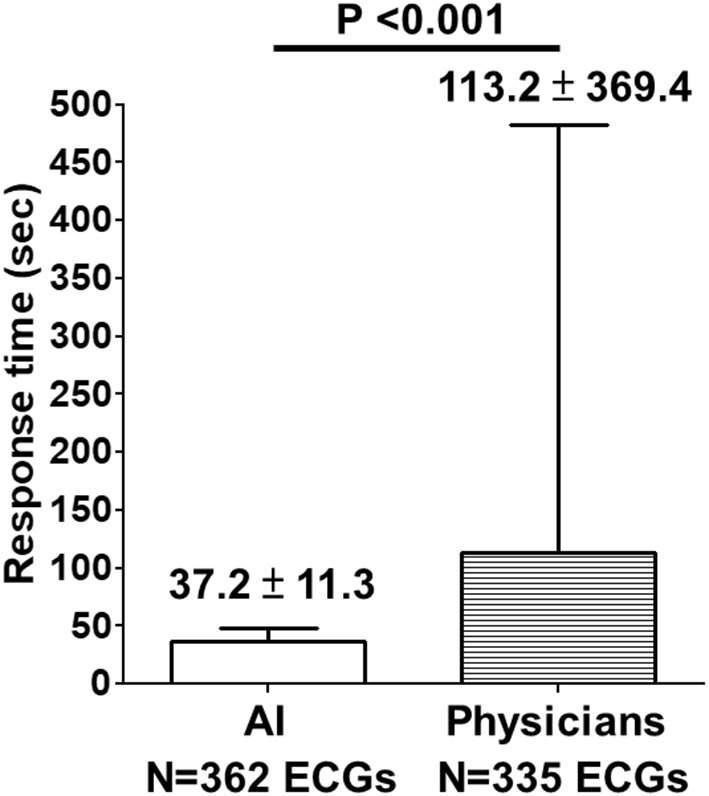
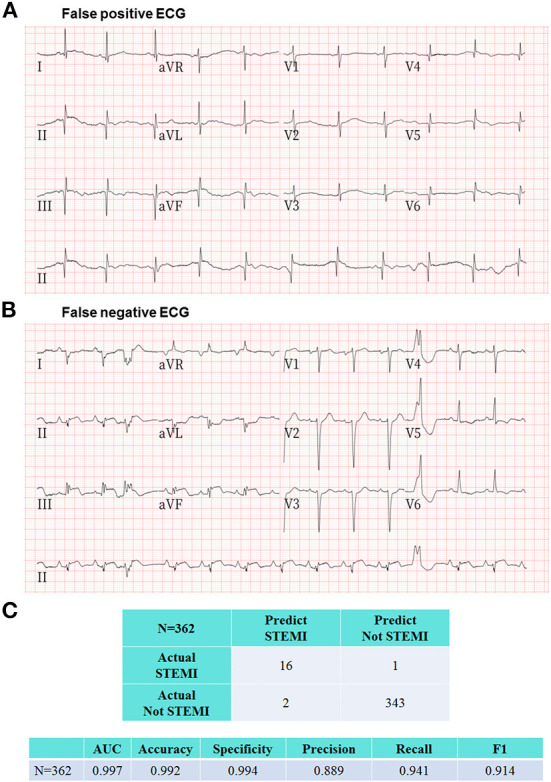
Results: Between July 17, 2021, and March 26, 2022, the AI model classified 362 prehospital 12-lead ECGs obtained from 275 consecutive patients who had called the 119 dispatch centers of fire stations in Central Taiwan for symptoms of chest pain or shortness of breath. The AI's response time to the EMTs in ambulance vehicles was 37.2 ± 11.3 s, which was shorter than the online physicians' response time from 11 other fire stations with no AI implementation (113.2 ± 369.4 s, P < 0.001) after analyzing another set of 335 prehospital 12-lead ECGs. The evaluation metrics including accuracy, precision, specificity, recall, area under the receiver operating characteristic curve, and F1 score to assess the overall AI performance in the remote detection of STEMI were 0.992, 0.889, 0.994, 0.941, 0.997, and 0.914, respectively. During the study period, the AI model promptly identified 10 STEMI patients who underwent primary percutaneous coronary intervention (PPCI) with a median contact-to-door time of 18.5 (IQR: 16-20.8) minutes.
Conclusion: Implementation of an all-day real-time AI-assisted remote detection of STEMI on prehospital 12-lead ECGs in the field is feasible with a high diagnostic accuracy rate. This approach may help minimize preventable delays in contact-to-treatment times for STEMI patients who require PPCI.
Keywords: ST-elevation myocardial infarction (STEMI); artificial intelligence (AI); contact-to-balloon (C2B) time; convolutional neural network and long short-term memory (CNN-LSTM); prehospital 12-lead ECGs.
Copyright © 2022 Chen, Wang, Liu, Tsai, Wu, Hsieh, Wei, Shih, Shiao, Hwang, Wu, Hsu and Chang.
Conflict of interest statement
Author P-HH was employed by Ever Fortune AI Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Implementation of an All-Day Artificial Intelligence-Based Triage System to Accelerate Door-to-Balloon Times.Mayo Clin Proc. 2022 Dec;97(12):2291-2303. doi: 10.1016/j.mayocp.2022.05.014. Epub 2022 Nov 3. Mayo Clin Proc. 2022. PMID: 36336511
-
Corrigendum: Artificial intelligence-assisted remote detection of ST-elevation myocardial infarction using a mini-12-lead electrocardiogram device in prehospital ambulance care.Front Cardiovasc Med. 2022 Dec 9;9:1078223. doi: 10.3389/fcvm.2022.1078223. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36568545 Free PMC article.
-
Diversion of ST-elevation myocardial infarction patients for primary angioplasty based on wireless prehospital 12-lead electrocardiographic transmission directly to the cardiologist's handheld computer: a progress report.J Electrocardiol. 2005 Oct;38(4 Suppl):194-8. doi: 10.1016/j.jelectrocard.2005.06.035. J Electrocardiol. 2005. PMID: 16226101
-
Prehospital 12-lead electrocardiogram for patients with chest pain: a pilot study.Hong Kong Med J. 2018 Oct;24(5):484-491. doi: 10.12809/hkmj177135. Hong Kong Med J. 2018. PMID: 30262677 Review.
-
Context-independent identification of myocardial ischemia in the prehospital ECG of chest pain patients.J Electrocardiol. 2024 Jan-Feb;82:34-41. doi: 10.1016/j.jelectrocard.2023.10.009. Epub 2023 Nov 7. J Electrocardiol. 2024. PMID: 38006762 Review.
Cited by
-
A Novel Algorithm for Improving the Prehospital Diagnostic Accuracy of ST-Segment Elevation Myocardial Infarction.Prehosp Disaster Med. 2024 Feb;39(1):37-44. doi: 10.1017/S1049023X23006635. Epub 2023 Dec 4. Prehosp Disaster Med. 2024. PMID: 38047380 Free PMC article.
-
Impact of treatment management on the hospital stay in patients with acute coronary syndrome.BMC Cardiovasc Disord. 2024 Nov 9;24(1):630. doi: 10.1186/s12872-024-04304-0. BMC Cardiovasc Disord. 2024. PMID: 39522008 Free PMC article.
-
An Artificial Intelligence Analysis of Electrocardiograms for the Clinical Diagnosis of Cardiovascular Diseases: A Narrative Review.J Clin Med. 2024 Feb 11;13(4):1033. doi: 10.3390/jcm13041033. J Clin Med. 2024. PMID: 38398346 Free PMC article. Review.
-
Clinical Research in Prehospital Care: Current and Future Challenges.Clin Pract. 2023 Oct 23;13(5):1266-1285. doi: 10.3390/clinpract13050114. Clin Pract. 2023. PMID: 37887090 Free PMC article. Review.
-
Identifying and Solving Gaps in Pre- and In-Hospital Acute Myocardial Infarction Care in Asia-Pacific Countries.Korean Circ J. 2023 Sep;53(9):594-605. doi: 10.4070/kcj.2023.0169. Korean Circ J. 2023. PMID: 37653695 Free PMC article. Review.
References
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, et al. . 2013 ACCF/AHA guideline for the management of St-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. (2013) 127:e362–425. 10.1161/CIR.0b013e3182742cf6 - DOI - PubMed
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. . 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-Segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018) 39:119–77. 10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Chang KC, Hsieh PH, Wu MY, Wang YC, Wei JT, Shih ESC, et al. . Usefulness of multi-labelling artificial intelligence in detecting rhythm disorders and acute ST-elevation myocardial infarction on 12-Lead electrocardiogram. Eur Heart J Digital Health. (2021) 2:299–310. 10.1093/ehjdh/ztab029 - DOI - PMC - PubMed
-
- Wang YC, Chen KW, Tsai BY, Wu MY, Hsieh PH, Wei JT, et al. . Implementation of an all-day artifical intelligence-based triage system to accelerate door-to-ballon times. Mayo Clinic Proc. (2022) (in press). - PubMed
LinkOut - more resources
Full Text Sources