

Interpretable machine learning for 28-day all-cause in-hospital mortality prediction in critically ill patients with heart failure combined with hypertension: A retrospective cohort study based on medical information mart for intensive care database-IV and eICU databases
- PMID: 36312291
- PMCID: PMC9597462
- DOI: 10.3389/fcvm.2022.994359
Interpretable machine learning for 28-day all-cause in-hospital mortality prediction in critically ill patients with heart failure combined with hypertension: A retrospective cohort study based on medical information mart for intensive care database-IV and eICU databases
Abstract
Background: Heart failure (HF) combined with hypertension is an extremely important cause of in-hospital mortality, especially for the intensive care unit (ICU) patients. However, under intense working pressure, the medical staff are easily overwhelmed by the large number of clinical signals generated in the ICU, which may lead to treatment delay, sub-optimal care, or even wrong clinical decisions. Individual risk stratification is an essential strategy for managing ICU patients with HF combined with hypertension. Artificial intelligence, especially machine learning (ML), can develop superior models to predict the prognosis of these patients. This study aimed to develop a machine learning method to predict the 28-day mortality for ICU patients with HF combined with hypertension.
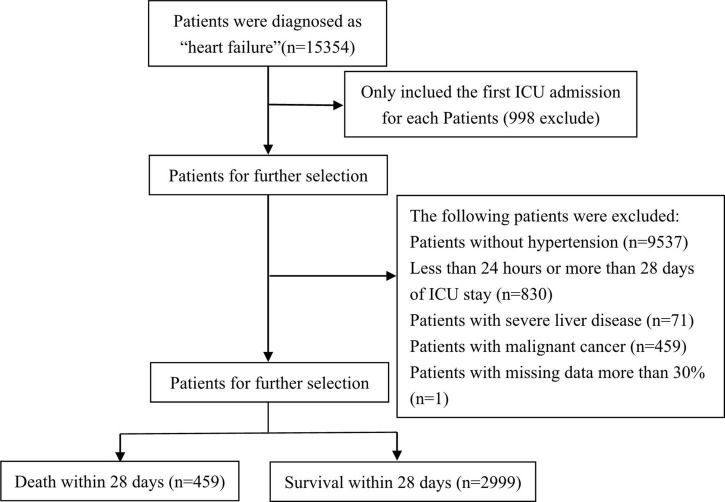
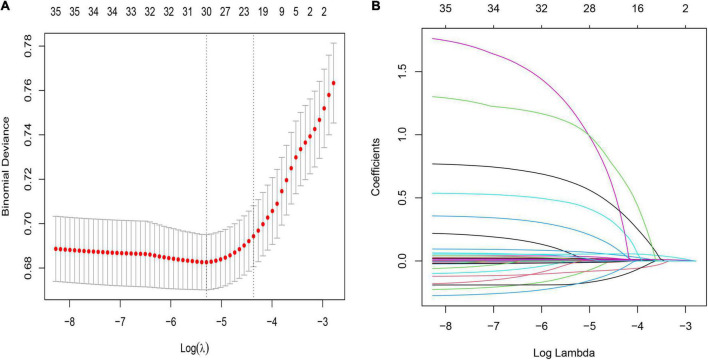
Methods: We enrolled all critically ill patients with HF combined with hypertension in the Medical Information Mart for IntensiveCare Database-IV (MIMIC-IV, v.1.4) and the eICU Collaborative Research Database (eICU-CRD) from 2008 to 2019. Subsequently, MIMIC-IV was divided into training cohort and testing cohort in an 8:2 ratio, and eICU-CRD was designated as the external validation cohort. The least absolute shrinkage and selection operator (LASSO) Cox regression with internal tenfold cross-validation was used for data dimension reduction and identifying the most valuable predictive features for 28-day mortality. Based on its accuracy and area under the curve (AUC), the best model in the validation cohort was selected. In addition, we utilized the Shapley Additive Explanations (SHAP) method to highlight the importance of model features, analyze the impact of individual features on model output, and visualize an individual's Shapley values.
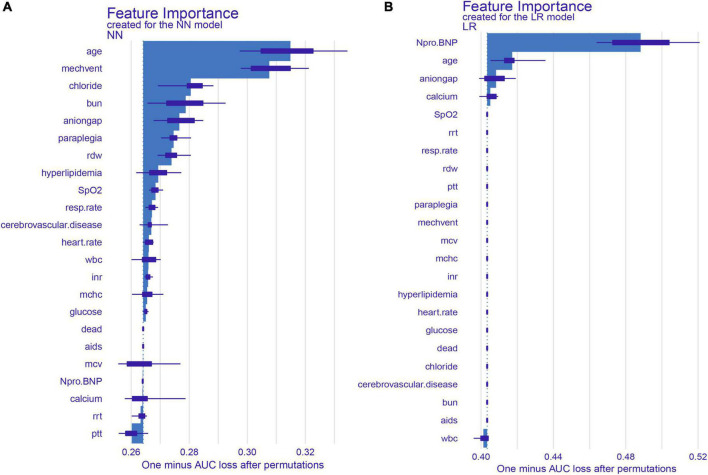
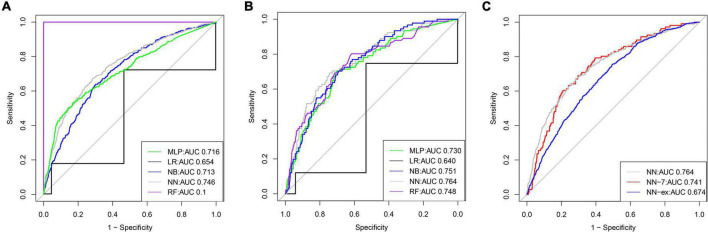
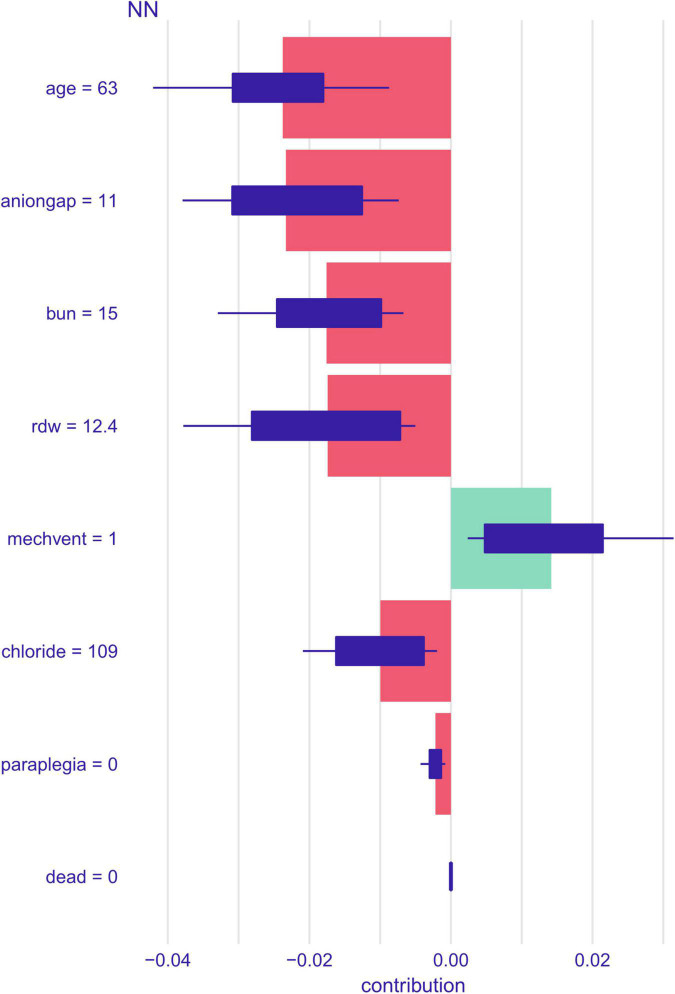
Results: A total of 3,458 and 6582 patients with HF combined with hypertension in MIMIC-IV and eICU-CRD were included. The patients, including 1,756 males, had a median (Q1, Q3) age of 75 (65, 84) years. After selection, 22 out of a total of 58 clinical parameters were extracted to develop the machine-learning models. Among four constructed models, the Neural Networks (NN) model performed the best predictive performance with an AUC of 0.764 and 0.674 in the test cohort and external validation cohort, respectively. In addition, a simplified model including seven variables was built based on NN, which also had good predictive performance (AUC: 0.741). Feature importance analysis showed that age, mechanical ventilation (MECHVENT), chloride, bun, anion gap, paraplegia, rdw (RDW), hyperlipidemia, peripheral capillary oxygen saturation (SpO2), respiratory rate, cerebrovascular disease, heart rate, white blood cell (WBC), international normalized ratio (INR), mean corpuscular hemoglobin concentration (MCHC), glucose, AIDS, mean corpuscular volume (MCV), N-terminal pro-brain natriuretic peptide (Npro. BNP), calcium, renal replacement therapy (RRT), and partial thromboplastin time (PTT) were the top 22 features of the NN model with the greatest impact. Finally, after hyperparameter optimization, SHAP plots were employed to make the NN-based model interpretable with an analytical description of how the constructed model visualizes the prediction of death.
Conclusion: We developed a predictive model to predict the 28-day mortality for ICU patients with HF combined with hypertension, which proved superior to the traditional logistic regression analysis. The SHAP method enables machine learning models to be more interpretable, thereby helping clinicians to better understand the reasoning behind the outcome and assess in-hospital outcomes for critically ill patients.
Keywords: MIMIC-IV; heart failure; hypertension; interpretable machine learning; neural networks.
Copyright © 2022 Peng, Huang, Liu, Deng, Sun, Tang, Chen, Cao, Wang, Duan, Luo and Peng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Interpretable machine learning for predicting 28-day all-cause in-hospital mortality for hypertensive ischemic or hemorrhagic stroke patients in the ICU: a multi-center retrospective cohort study with internal and external cross-validation.Front Neurol. 2023 Aug 8;14:1185447. doi: 10.3389/fneur.2023.1185447. eCollection 2023. Front Neurol. 2023. PMID: 37614971 Free PMC article.
-
Interpretable machine learning model for early prediction of 28-day mortality in ICU patients with sepsis-induced coagulopathy: development and validation.Eur J Med Res. 2024 Jan 3;29(1):14. doi: 10.1186/s40001-023-01593-7. Eur J Med Res. 2024. PMID: 38172962 Free PMC article.
-
Predicting sepsis in-hospital mortality with machine learning: a multi-center study using clinical and inflammatory biomarkers.Eur J Med Res. 2024 Mar 6;29(1):156. doi: 10.1186/s40001-024-01756-0. Eur J Med Res. 2024. PMID: 38448999 Free PMC article.
-
Artificial intelligence in clinical care amidst COVID-19 pandemic: A systematic review.Comput Struct Biotechnol J. 2021;19:2833-2850. doi: 10.1016/j.csbj.2021.05.010. Epub 2021 May 7. Comput Struct Biotechnol J. 2021. PMID: 34025952 Free PMC article. Review.
-
The CMLA score: A novel tool for early prediction of renal replacement therapy in patients with cardiogenic shock.Curr Probl Cardiol. 2024 Dec;49(12):102870. doi: 10.1016/j.cpcardiol.2024.102870. Epub 2024 Sep 27. Curr Probl Cardiol. 2024. PMID: 39343053 Review.
Cited by
-
Accounting for Red Cell Distribution Width Improves Risk Stratification by Commonly Used Mortality/Deterioration Risk Scores in Adult Patients Hospitalized Due to COVID-19.Life (Basel). 2024 Oct 5;14(10):1267. doi: 10.3390/life14101267. Life (Basel). 2024. PMID: 39459567 Free PMC article.
-
Development and Validation of Multimodal Models to Predict the 30-Day Mortality of ICU Patients Based on Clinical Parameters and Chest X-Rays.J Imaging Inform Med. 2024 Aug;37(4):1312-1322. doi: 10.1007/s10278-024-01066-1. Epub 2024 Mar 6. J Imaging Inform Med. 2024. PMID: 38448758 Free PMC article.
-
Developing a predictive nomogram for AMI in elderly patients with AHF: a retrospective analysis.Front Med (Lausanne). 2025 Jul 9;12:1555596. doi: 10.3389/fmed.2025.1555596. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40703271 Free PMC article.
-
Interpretability-based machine learning for predicting the risk of death from pulmonary inflammation in Chinese intensive care unit patients.Front Med (Lausanne). 2024 Jun 12;11:1399527. doi: 10.3389/fmed.2024.1399527. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38933112 Free PMC article.
-
Development and validation of a novel combinatorial nomogram model to predict in-hospital deaths in heart failure patients.BMC Cardiovasc Disord. 2024 Jan 3;24(1):16. doi: 10.1186/s12872-023-03683-0. BMC Cardiovasc Disord. 2024. PMID: 38172656 Free PMC article.
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1789–858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous