

Comprehensive assessments of pulmonary circulation in children with pulmonary hypertension associated with congenital heart disease
- PMID: 36313863
- PMCID: PMC9614099
- DOI: 10.3389/fped.2022.1011631
Comprehensive assessments of pulmonary circulation in children with pulmonary hypertension associated with congenital heart disease
Abstract
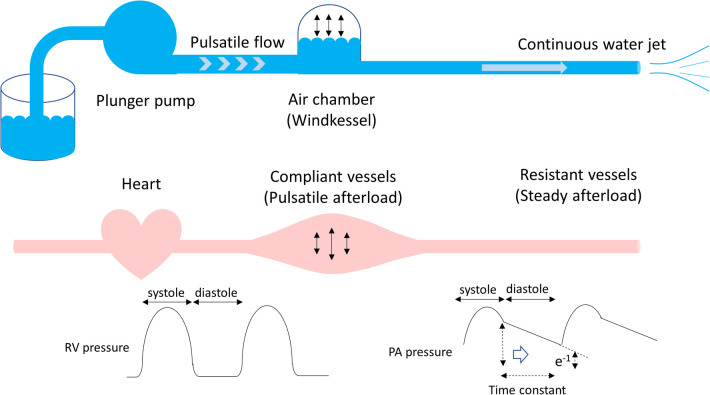
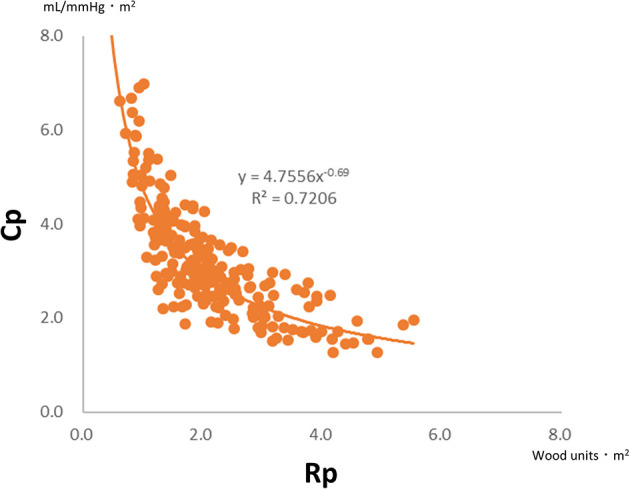
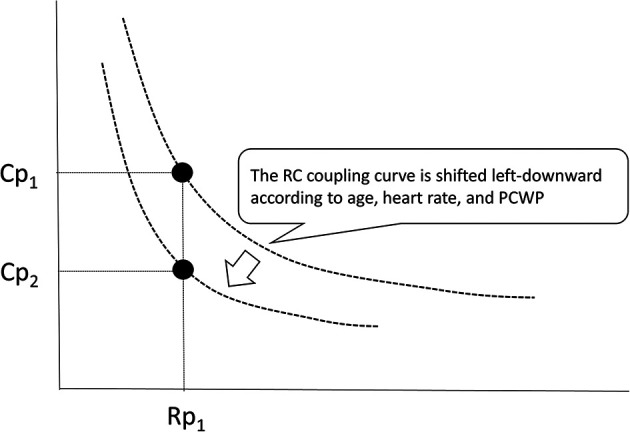
Pulmonary hypertension associated with congenital heart disease (CHD-PH) encompasses different conditions confounded by the left-to-right shunt, left heart obstruction, ventricular dysfunction, hypoxia due to airway obstruction, dysplasia/hypoplasia of the pulmonary vasculature, pulmonary vascular obstructive disease, and genetic variations of vasoactive mediators. Pulmonary input impedance consists of the pulmonary vascular resistance (Rp) and capacitance (Cp). Rp is calculated as the transpulmonary pressure divided by the pulmonary cardiac output, whereas Cp is calculated as the pulmonary stroke volume divided by the pulmonary arterial pulse pressure. The plots of Rp and Cp demonstrate a unique hyperbolic relationship, namely, the resistor-capacitor coupling curve, which represents the pulmonary vascular condition. The product of Rp and Cp is the exponential pressure decay, which refers to the time constant. Alterations in Cp are more considerable in CHD patients at an early stage of developing pulmonary hypertension or with excessive pulmonary blood flow due to a left-to-right shunt. The importance of Cp has gained attention because recent reports have shown that low Cp potentially reflects poor prognosis in patients with CHD-PH and idiopathic pulmonary hypertension. It is also known that Cp levels decrease in specific populations, such as preterm infants and trisomy 21. Therefore, both Rp and Cp should be individually evaluated in the management of children with CHD-PH who have different disease conditions.
Keywords: pulmonary arterial capacitance; pulmonary arterial compliance; pulmonary arterial hypertension; pulmonary vascular resistance; resistor–capacitor time; time constant (tau).
© 2022 Muneuchi, Ezaki, Sugitani and Watanabe.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J. (2009) 30:2493–537. 10.1093/eurheartj/ehp297 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous