

A Randomized, Controlled Trial of Resistance Training Added to Caloric Restriction Plus Aerobic Exercise Training in Obese Heart Failure With Preserved Ejection Fraction
- PMID: 36314122
- PMCID: PMC9974606
- DOI: 10.1161/CIRCHEARTFAILURE.122.010161
A Randomized, Controlled Trial of Resistance Training Added to Caloric Restriction Plus Aerobic Exercise Training in Obese Heart Failure With Preserved Ejection Fraction
Abstract
Background: We have shown that combined caloric restriction (CR) and aerobic exercise training (AT) improve peak exercise O2 consumption (VO2peak), and quality-of-life in older patients with obese heart failure with preserved ejection fraction. However, ≈35% of weight lost during CR+AT was skeletal muscle mass. We examined whether addition of resistance training (RT) to CR+AT would reduce skeletal muscle loss and further improve outcomes.
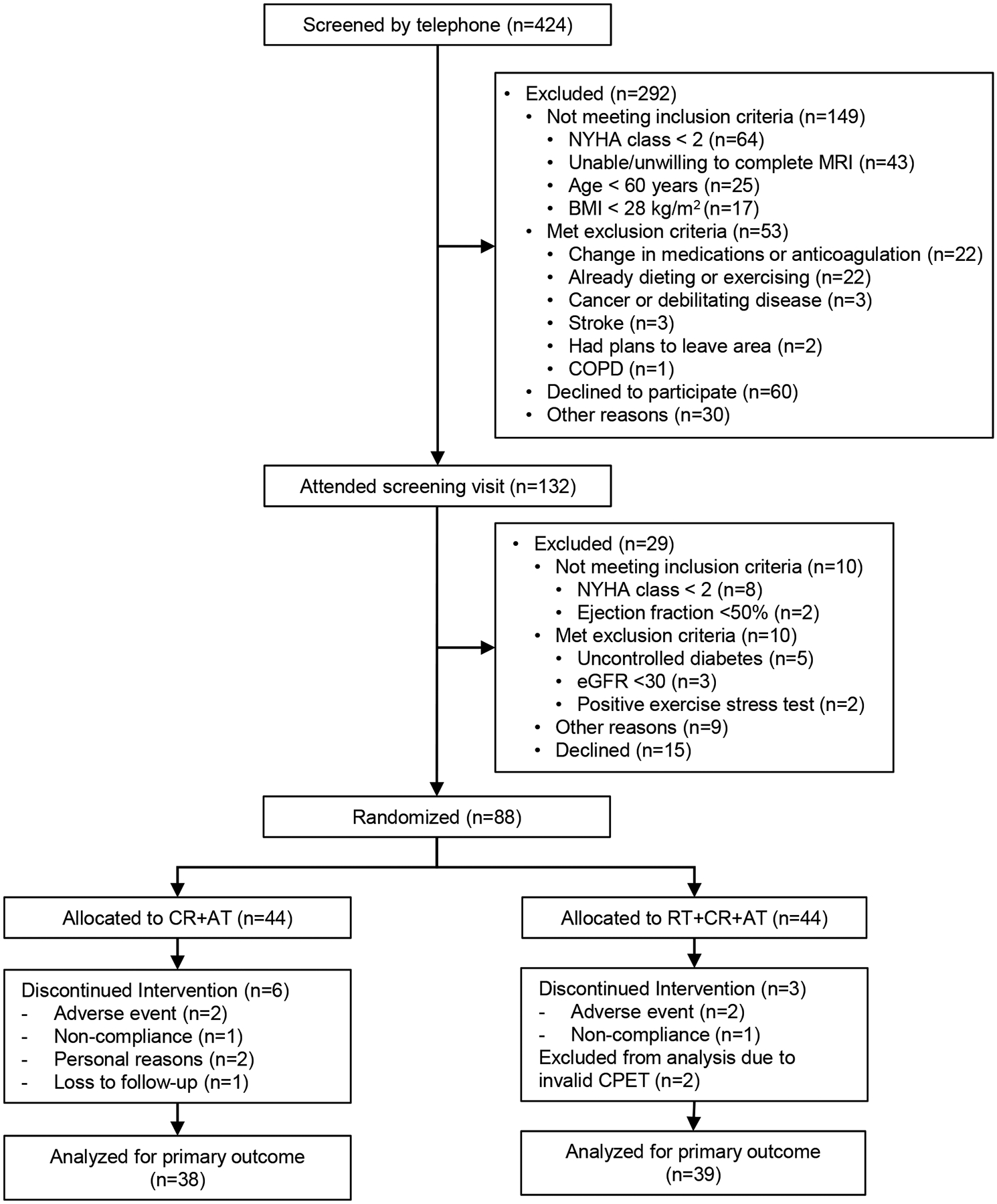
Methods: This study is a randomized, controlled, single-blind, 20-week trial of RT+CR+AT versus CR+AT in 88 patients with chronic heart failure with preserved ejection fraction and body mass index (BMI) ≥28 kg/m2. Outcomes at 20 weeks included the primary outcome (VO2peak); MRI and dual X-ray absorptiometry; leg muscle strength and quality (leg strength ÷ leg skeletal muscle area); and Kansas City Cardiomyopathy Questionnaire.
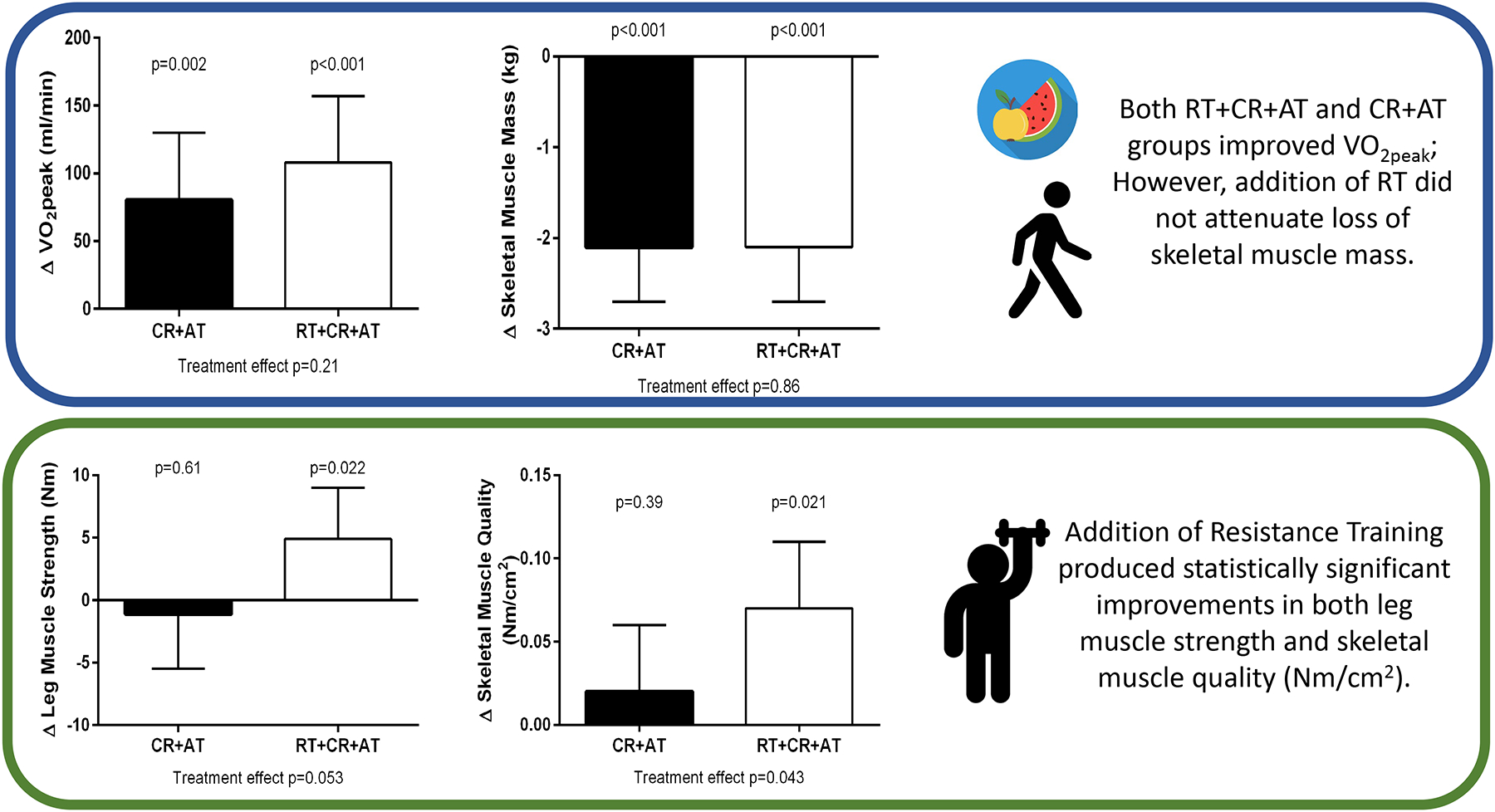
Results: Seventy-seven participants completed the trial. RT+CR+AT and CR+AT produced nonsignificant differences in weight loss: mean (95% CI): -8 (-9, -7) versus -9 (-11, -8; P=0.21). RT+CR+AT and CR+AT had non-significantly differences in the reduction of body fat [-6.5 (-7.2, -5.8) versus -7.4 (-8.1, -6.7) kg] and skeletal muscle [-2.1 (-2.7, -1.5) versus -2.1 (-2.7, -1.4) kg] (P=0.20 and 0.23, respectively). RT+CR+AT produced significantly greater increases in leg muscle strength [4.9 (0.7, 9.0) versus -1.1 (-5.5, 3.2) Nm, P=0.05] and leg muscle quality [0.07 (0.03, 0.11) versus 0.02 (-0.02, 0.06) Nm/cm2, P=0.04]. Both RT+CR+AT and CR+AT produced significant improvements in VO2peak [108 (958, 157) versus 80 (30, 130) mL/min; P=0.001 and 0.002, respectively], and Kansas City Cardiomyopathy Questionnaire score [17 (12, 22) versus 23 (17, 28); P=0.001 for both], with no significant between-group differences. Both RT+CR+AT and CR+AT significantly reduced LV mass and arterial stiffness. There were no study-related serious adverse events.
Conclusions: In older obese heart failure with preserved ejection fraction patients, CR+AT produces large improvements in VO2peak and quality-of-life. Adding RT to CR+AT increased leg strength and muscle quality without attenuating skeletal muscle loss or further increasing VO2peak or quality-of-life.
Registration: URL: https://ClincalTrials.gov; Unique identifier: NCT02636439.
Keywords: diastolic heart failure; elderly; exercise; heart failure; obesity; resistance training.
Figures
Comment in
-
Response by Brubaker et al to Letter Regarding "A Randomized, Controlled Trial of Resistance Training Added to Caloric Restriction Plus Aerobic Exercise Training in Obese Heart Failure With Preserved Ejection Fraction".Circ Heart Fail. 2023 May;16(5):e010419. doi: 10.1161/CIRCHEARTFAILURE.123.010419. Epub 2023 Apr 18. Circ Heart Fail. 2023. PMID: 37070429 Free PMC article. No abstract available.
References
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation. 2022;145: e153–e639 - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure. J AmColl Cardiol. 2013;62(16):e147–e239.. - PubMed
-
- Owan TE, Hodge DO, Herges RM, et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006; 355:251–259. - PubMed
-
- Kitzman DW, Gardin JM, Gottdiener JS, et al. Importance of heart failure with preserved systolic function in patients > or = 65 years of age. CHS Research Group. Cardiovascular Health Study. Am J Cardiol. 2001; 87:413–419. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
