

In-Hospital Virtual Peer-to-Peer Consultation to Increase Guideline-Directed Medical Therapy for Heart Failure: A Pilot Randomized Trial
- PMID: 36314130
- PMCID: PMC9974597
- DOI: 10.1161/CIRCHEARTFAILURE.122.010158
In-Hospital Virtual Peer-to-Peer Consultation to Increase Guideline-Directed Medical Therapy for Heart Failure: A Pilot Randomized Trial
Abstract
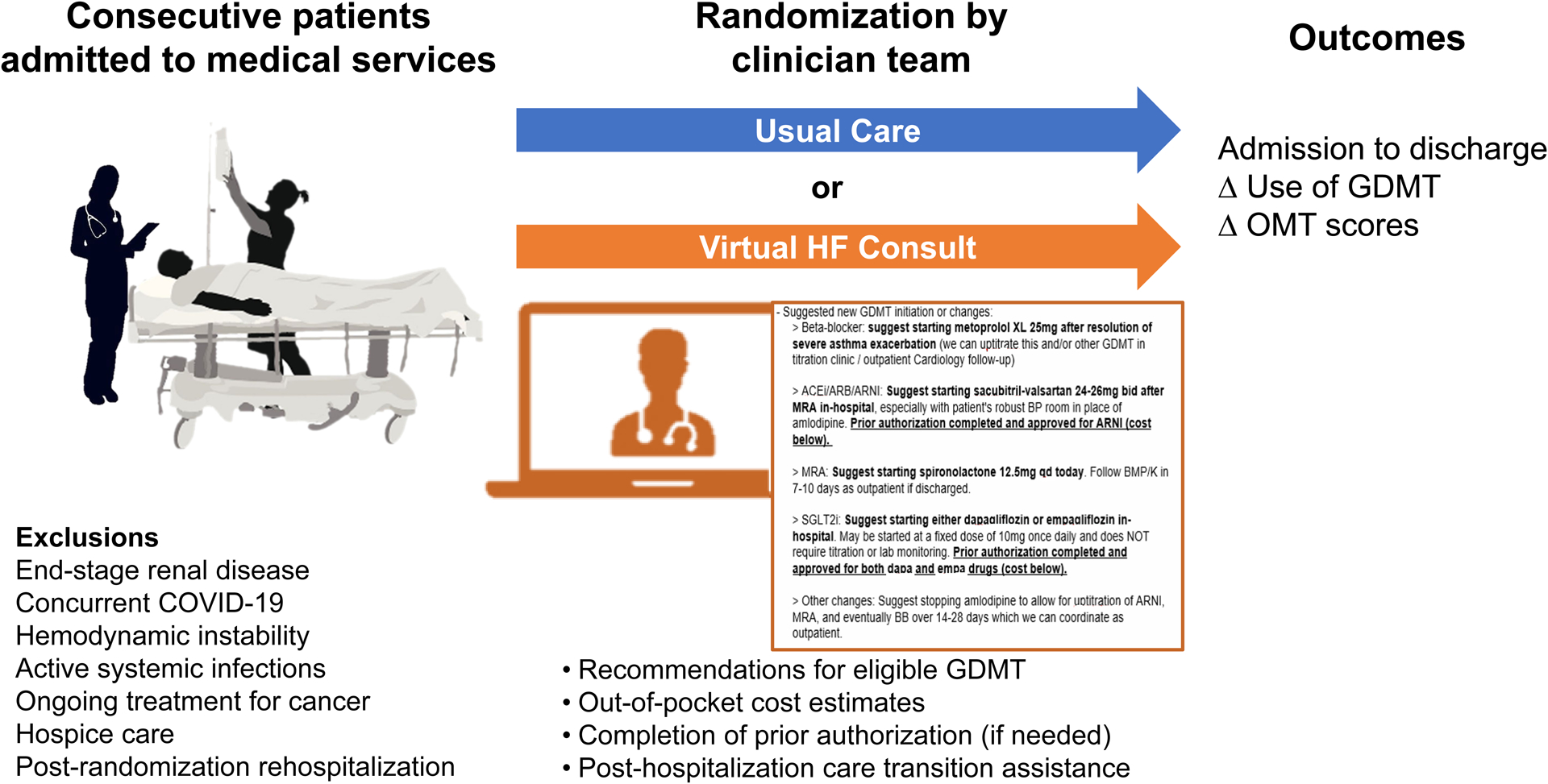
Background: Guideline-directed medical therapy (GDMT) for heart failure with reduced ejection fraction (HFrEF) improves clinical outcomes and quality of life. Optimizing GDMT in the hospital is associated with greater long-term use in HFrEF. This study aimed to describe the efficacy of a multidisciplinary virtual HF intervention on GDMT optimization among patients with HFrEF admitted for any cause.
Methods: In this pilot randomized, controlled study, consecutive patients with HFrEF admitted to noncardiology medicine services for any cause were identified at a large academic tertiary care hospital between May to September 2021. Major exclusions were end-stage renal disease, hemodynamic instability, concurrent COVID-19 infection, and current enrollment in hospice care. Patients were randomized to a clinician-level virtual peer-to-peer consult intervention providing GDMT recommendations and information on medication costs versus usual care. Primary end points included (1) proportion of patients with new GDMT initiation or use and (2) changes to HF optimal medical therapy scores which included target dosing (range, 0-9).
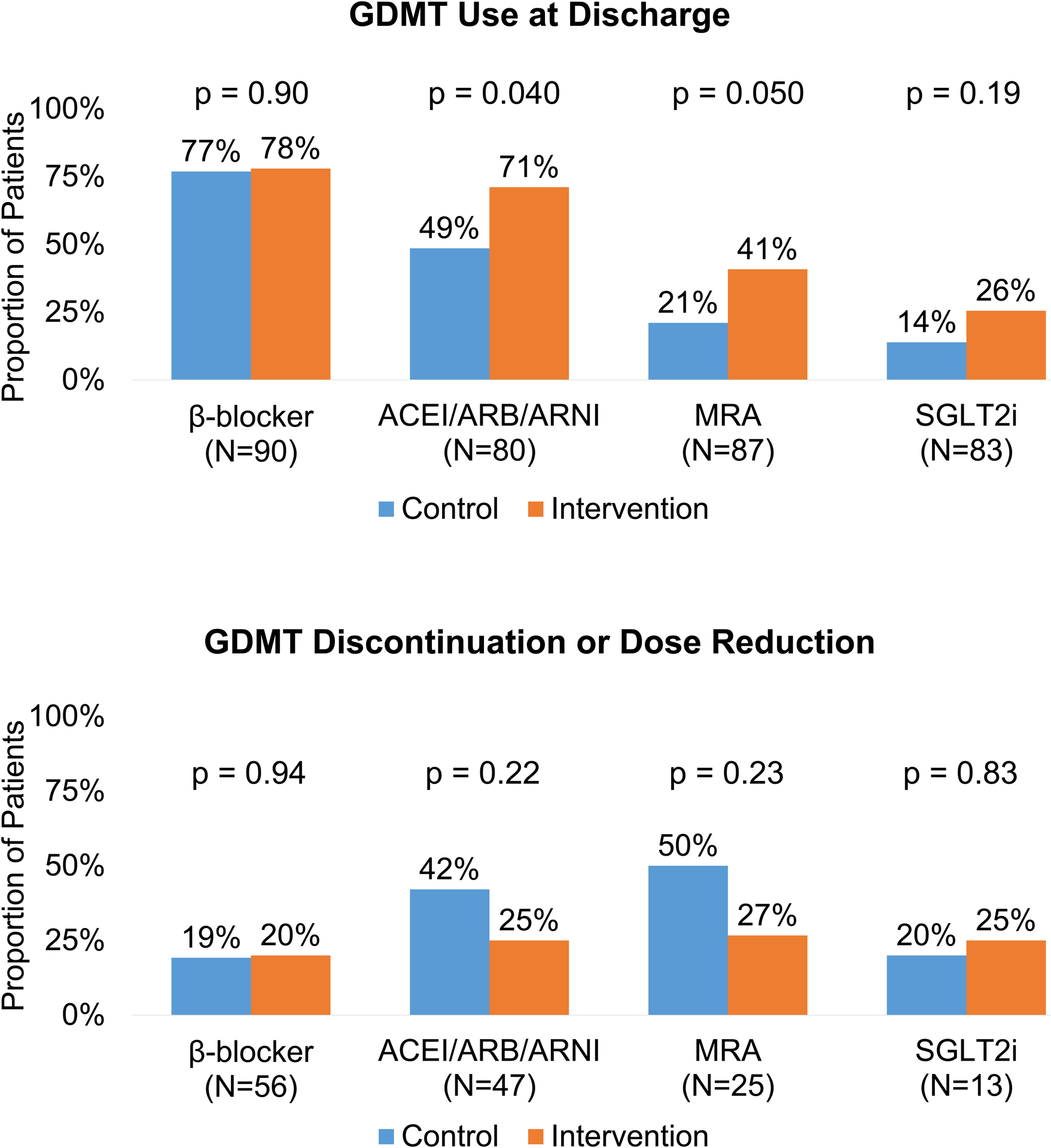
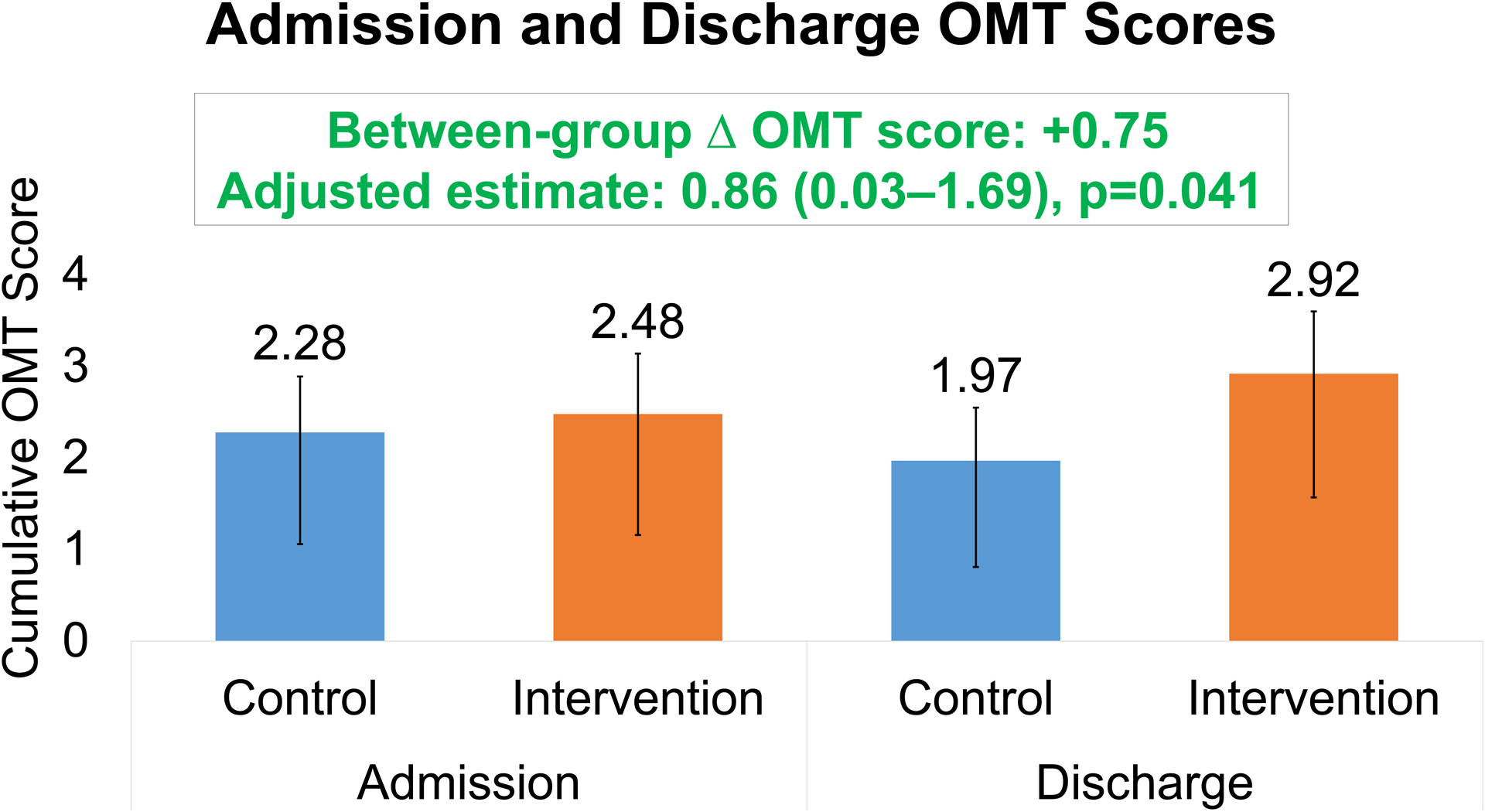
Results: Of 242 patients identified, 91 (38%) were eligible and randomized to intervention (N=52) or usual care (N=39). Baseline characteristics were similar between intervention and usual care (mean age 63 versus 67 years, 23% versus 26% female, 46% versus 49% Black, mean ejection fraction 33% versus 31%). GDMT use on admission was also similar. There were greater proportions of patients with GDMT initiation or continuation with the intervention compared with usual care. After adjusting for optimal medical therapy score on admission, changes to optimal medical therapy score at discharge were higher for the intervention group compared with usual care (+0.44 versus -0.31, absolute difference +0.75, adjusted estimate 0.86±0.42; P=0.041).
Conclusions: Among eligible patients with HFrEF hospitalized for any cause on noncardiology services, a multidisciplinary pilot virtual HF consultation increased new GDMT initiation and dose optimization at discharge.
Keywords: heart failure; hospitalization; practice patterns, physicians'; quality of care; remote consultation.
Figures
References
-
- Greene SJ, O’Brien EC, Mentz RJ, Luo N, Hardy NC, Laskey WK, Heidenreich PA, Chang CL, Turner SJ, Yancy CW, et al. Home-Time After Discharge Among Patients Hospitalized With Heart Failure. Journal of the American College of Cardiology. 2018;71:2643–2652. doi: 10.1016/j.jacc.2018.03.517 - DOI - PMC - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6:606–619. doi: 10.1161/HHF.0b013e318291329a - DOI - PMC - PubMed
-
- Allen LA, Gheorghiade M, Reid KJ, Dunlay SM, Chan PS, Hauptman PJ, Zannad F, Konstam MA, Spertus JA. Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life. Circ Cardiovasc Qual Outcomes. 2011;4:389–398. doi: 10.1161/CIRCOUTCOMES.110.958009 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
