

Non-biologic, steroid-sparing therapies for non-infectious intermediate, posterior, and panuveitis in adults
- PMID: 36315029
- PMCID: PMC9621106
- DOI: 10.1002/14651858.CD014831.pub2
Non-biologic, steroid-sparing therapies for non-infectious intermediate, posterior, and panuveitis in adults
Abstract
Background: Non-infectious intermediate, posterior, and panuveitis (NIIPPU) represent a heterogenous collection of autoimmune and inflammatory disorders isolated to or concentrated in the posterior structures of the eye. Because NIIPPU is typically a chronic condition, people with NIIPPU frequently require treatment with steroid-sparing immunosuppressive therapy. Methotrexate, mycophenolate, cyclosporine, azathioprine, and tacrolimus are non-biologic, disease-modifying antirheumatic drugs (DMARDs) which have been used to treat people with NIIPPU.
Objectives: To compare the effectiveness and safety of selected DMARDs (methotrexate, mycophenolate mofetil, tacrolimus, cyclosporine, and azathioprine) in the treatment of NIIPPU in adults.
Search methods: We searched CENTRAL (which contains the Cochrane Eyes and Vision Trials Register), MEDLINE, Embase, the Latin American and Caribbean Health Sciences database, ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform, most recently on 16 April 2021.
Selection criteria: We included randomized controlled trials (RCTs) comparing selected DMARDs (methotrexate, mycophenolate, tacrolimus, cyclosporine, and azathioprine) with placebo, standard of care (topical steroids, with or without oral steroids), or with each other.
Data collection and analysis: We used standard methodological procedures expected by Cochrane.
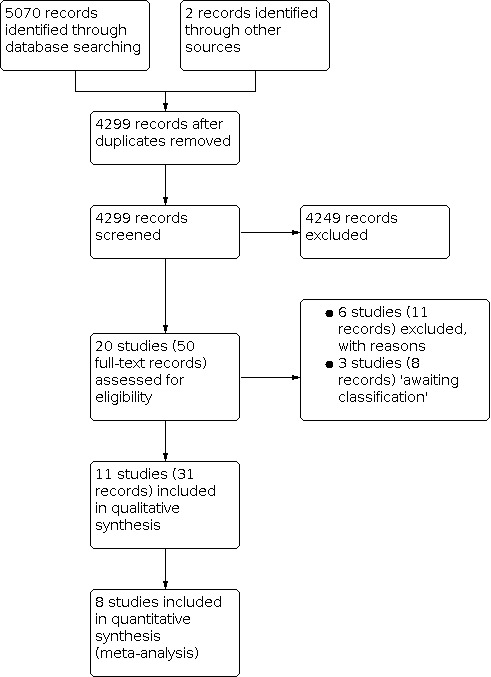
Main results: We included 11 RCTs with a total of 601 participants in this review. DMARDs versus control Two studies compared an experimental DMARD (cyclosporine A or enteric-coated mycophenolate [EC-MPS]) plus oral steroid with steroid monotherapy. We did not pool these results into a meta-analysis because the dose of cyclosporine used was much higher than that used in current clinical practice. The evidence is very uncertain about whether EC-MPS plus low-dose oral steroid results in a higher proportion of participants achieving control of inflammation over steroid monotherapy (risk ratio [RR] 2.81, 95% confidence interval [CI] 1.10 to 7.17; 1 study, 41 participants; very low-certainty evidence). The change in best-corrected visual acuity (BCVA) was reported separately for right and left eyes. The evidence for improvement (lower logarithm of the minimum angle of resolution (logMAR) indicates better vision) between the groups is very uncertain (mean difference [MD] -0.03 and -0.10, 95% CI -0.96 to 0.90 and -0.27 to 0.07 for right and left, respectively; 1 study, 82 eyes; very low-certainty evidence). No data were available for the following outcomes: proportion of participants achieving a 2-line improvement in visual acuity, with confirmed macular edema, or achieving steroid-sparing control. The evidence for the proportion of participants requiring cessation of medication in the DMARD versus control group is very uncertain (RR 2.61, 95% CI 0.11 to 60.51; 1 study, 41 participants; very low-certainty evidence). Methotrexate versus mycophenolate We were able to combine two studies into a meta-analysis comparing methotrexate versus mycophenolate mofetil. Methotrexate probably results in a slight increase in the proportion of participants achieving control of inflammation, including steroid-sparing control, compared to mycophenolate at six months (RR 1.23, 95% CI 1.01 to 1.50; 2 studies, 261 participants; moderate-certainty evidence). Change in BCVA was reported per eye and the treatments likely result in little to no difference in change in vision (MD 0.01 logMAR higher [worse] for methotrexate versus mycophenolate; 2 studies, 490 eyes; moderate-certainty evidence). No data were available for the proportion of participants achieving a 2-line improvement in visual acuity. The evidence is very uncertain regarding the proportion of participants with confirmed macular edema between methotrexate versus mycophenolate (RR 0.49, 95% CI 0.19 to 1.30; 2 studies, 35 eyes; very low-certainty). Methotrexate versus mycophenolate may result in little to no difference in the proportion of participants requiring cessation of medication (RR 0.99, 95% CI 0.43 to 2.27; 2 studies, 296 participants; low-certainty evidence). Steroids with or without azathioprine versus cyclosporine A Four studies compared steroids with or without azathioprine (oral steroids, intravenous [IV] steroids, or azathioprine) to cyclosporine A. We excluded two studies from the meta-analysis because the participants were treated with 8 mg to 15 mg/kg/day of cyclosporine A, a significantly higher dose than is utilized today because of concerns for nephrotoxicity. The remaining two studies were conducted in all Vogt-Koyanagi-Harada disease (VKH) populations and compared cyclosporine A to azathioprine or IV pulse-dose steroids. The evidence is very uncertain for whether the steroids with or without azathioprine or cyclosporine A influenced the proportion of participants achieving control of inflammation (RR 0.84, 95% CI 0.70 to 1.02; 2 studies, 112 participants; very low-certainty evidence), achieving steroid-sparing control (RR 0.64, 95% CI 0.33 to 1.25; 1 study, 21 participants; very low-certainty evidence), or requiring cessation of medication (RR 0.85, 95% 0.21 to 3.45; 2 studies, 91 participants; very low-certainty evidence). The evidence is uncertain for improvement in BCVA (MD 0.04 logMAR lower [better] with the steroids with or without azathioprine versus cyclosporine A; 2 studies, 91 eyes; very low-certainty evidence). There were no data available (with current cyclosporine A dosing) for the proportion of participants achieving a 2-line improvement in visual acuity or with confirmed macular edema. Studies not included in synthesis We were unable to include three studies in any of the comparisons (in addition to the aforementioned studies excluded based on historic doses of cyclosporine A). One was a dose-response study comparing cyclosporine A to cyclosporine G, a formulation which was never licensed and is not clinically available. We excluded another study from meta-analysis because it compared cyclosporine A and tacrolimus, considered to be of the same class (calcineurin inhibitors). We were unable to combine the third study, which examined tacrolimus monotherapy versus tacrolimus plus oral steroid, with any group.
Authors' conclusions: There is a paucity of data regarding which DMARD is most effective or safe in NIIPPU. Studies in general were small, heterogenous in terms of their design and outcome measures, and often did not compare different classes of DMARD with each other. Methotrexate is probably slightly more efficacious than mycophenolate in achieving control of inflammation, including steroid-sparing control (moderate-certainty evidence), although there was insufficient evidence to prefer one medication over the other in the VKH subgroup (very low-certainty evidence). Methotrexate may result in little to no difference in safety outcomes compared to mycophenolate.
Copyright © 2022 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
REM: none known.
TL: serves as the Principal Investigator for Cochrane Eyes and Vision US Satellite, which is support by grant UG1 EY020522 from the National Eye Institute, National Institutes of Health, USA.
PMcC: work undertaken as part of a postdoctoral research fellowship which is supported by Cochrane Eyes and Vision US Satellite (Grant UG1 EY020522), from the National Eye Institute, National Institutes of Health, USA.
LL: reports a grant from the National Eye Institute, National Institutes of Health, USA; payment to institution.
ASC: none.
AP: serves as a Co‐investigator for Cochrane Eyes and Vision US Satellite, which is support by grant UG1 EY020522 from the National Eye Institute, National Institutes of Health, USA.
Figures



































Update of
References
References to studies included in this review
Cuchacovich 2010 {published data only}
-
- Cuchacovich M, Solanes F, Díaz G, Cermenati T, Avila S, Verdaguer J, et al. Comparison of the clinical efficacy of two different immunosuppressive regimens in patients with chronic vogt-koyanagi-harada disease. Ocular Immunology and Inflammation 2010;18(3):200‐7. [CENTRAL: CN-00781196] [DOI: 10.3109/09273941003587541] - DOI - PubMed
Deuter 2018 {published data only}
-
- Deuter C, Engelmann K, Heiligenhaus A, Lanzl I, Mackensen F, Ness T, et al. Enteric-coated mycophenolate sodium in the treatment of non-infectious intermediate uveitis: results of a prospective, controlled, randomised, open-label, early terminated multicentre trial. British Journal of Ophthalmology 2018;102(5):647‐53. [CENTRAL: CN-00781196] [DOI: 10.1136/bjophthalmol-2017-310156] - DOI - PubMed
-
- EUCTR2009-009998-10-DE. Myfortic (enteric-coated mycophenolate sodium) for the treatment of non-infectous intermediate uveitis – a prospective, controlled randomized multicenter trial. clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2009-00... (first received 2 December 2009).
-
- NCT01092533. Myfortic for the treatment of non-infectious intermediate uveitis (MYCUV-IIT02) [Myfortic (enteric-coated mycophenolate sodium) for the treatment of non-infectious intermediate uveitis - a prospective, controlled randomized multicenter trial]. clinicaltrials.gov/ct2/show/study/NCT01092533 (first received 25 March 2010).
De Vries 1990 {published data only}
Lee 2012 {published data only}
-
- ISRCTN46576063. Tacrolimus monotherapy for uveitis [Dual steroid and tacrolimus therapy versus steroid withdrawal and tacrolimus therapy in the treatment of posterior segment intraocular inflammation (uveitis)]. trialsearch.who.int/Trial2.aspx?TrialID=ISRCTN46576063 (first received 16 April 2008). [DOI: ]
-
- Lee RW, Greenwood R, Amer R, Biester S, Plskova J, Forrester JV, et al. Tacrolimus monotherapy versus tacrolimus and prednisone for the maintenance of disease remission in non-infectious posterior segment intraocular inflammation. Investigative Ophthalmology and Visual Science 2009;50(13):2024.
Murphy 2005 {published data only}
Nussenblatt 1991 {published data only}
-
- Nussenblatt RB, Palestine A, Chan CC, Fujikawa LS, Stevens G, Green SB. A randomised, double-masked trial of sandimmune vs. prednisolone for endogenous uveitis. American Academy of Ophthalmology 1990;112:105. [CENTRAL: CN-00485269] - PubMed
-
- Nussenblatt RB, Palestine AG, Chan CC, Stevens G, Mellow SD, Green SB. Randomized, double-masked study of cyclosporine compared to prednisolone in the treatment of endogenous uveitis. American Journal of Ophthalmology 1991;112(2):138‐46. [CENTRAL: CN-00077346] [DOI: 10.1016/s0002-9394(14)76692-9] - DOI - PubMed
Nussenblatt 1993 {published data only}
-
- Nussenblatt RB, De Smet MD, Rubin B, Freidlin V, Whitcup SM, Davis J, et al. A masked, randomized, dose-response study between cyclosporine A and G in the treatment of sight-threatening uveitis of noninfectious origin. American Journal of Ophthalmology 1993;115(5):583‐91. [CENTRAL: CN-00093004] [DOI: 10.1016/s0002-9394(14)71454-0] - DOI - PubMed
Ono 2021 {published data only}
-
- JPRN-UMIN000014387. A prospective multicenter comparative clinical trial between corticosteroid pulse therapy vs. combination therapy of oral corticosteroid and cyclosporine on Vogt-Koyanagi-Harada disease. www.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000014387 (first received 27 June 2014). [CENTRAL: CN-01827271]
-
- Ono T, Goto H, Sakai T, Nitta F, Mizuki N, Takase H, et al. Comparison of combination therapy of prednisolone and cyclosporine with corticosteroid pulse therapy in Vogt–Koyanagi–Harada disease. Japanese Journal of Ophthalmology 2021 Oct 24 [Epub ahead of print]. [DOI: 10.1007/s10384-021-00878-w] - DOI - PubMed
-
- Ono T, Mochizuki M, Goto H, Sakai T, Nitta F, Mizuki N, et al. A prospective multi-center randomized clinical study comparing steroid-pulse therapy and a combined therapy with oral prednisolone and cyclosporine for new-onset acute Vogt-Koyanagi-Harada disease. Investigative Ophthalmology and Visual Science 2020;61(7):3169. [CENTRAL: CN-02179109] [EMBASE: 632697033]
Rathinam 2014 {published data only}
-
- NCT01232920. First-line antimetabolites as steroid-sparing treatment uveitis pilot trial. clinicaltrials.gov/ct2/show/NCT01232920 (first received 2 November 2010). [CENTRAL: CN-02032098]
-
- Niemeyer KM, Gonzales JA, Rathinam SR, Babu M, Thundikandy R, Kanakath A, et al. Quality-of-life outcomes from a randomized clinical trial comparing antimetabolites for intermediate, posterior, and panuveitis. American Journal of Ophthalmology 2017;179:10‐17. [CENTRAL: CN-01374518] [DOI: 10.1016/j.ajo.2017.04.003] - DOI - PMC - PubMed
-
- Niemeyer KM, Gonzales JA, Rathinam SR, Babu M, Thundikandy R, Kanakath A, et al. Quality of life outcomes from a randomized controlled trial comparing methotrexate to mycophenolate mofetil for noninfectious uveitis. Investigative Ophthalmology and Visual Science 2017;58(8):2174. [CENTRAL: CN-01616554] [EMBASE: 621489608]
-
- Shen E, Rathinam SR, Babu M, Browne E, Weinrib R, Porco T, et al. Uveitic macular edema outcomes: results of a randomized controlled trial. Clinical and Translational Science 2014;7(3):236. [CENTRAL: CN-01049997] [DOI: 10.1111/cts.12171] [EMBASE: 71734851] - DOI
Rathinam 2019 {published data only}
-
- CTRI 2017/09/009699. Immunosuppresants comparison for UVEITIS [First-line Antimetabolites as Steroid-sparing Treatment (FAST) Uveitis Trial]. ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=13782 (first received 9 November 2017).
-
- Kelly NK, Chattopadhyay A, Rathinam SR, Gonzales JA, Thundikandy R, Kanakath A, et al. Health- and vision-related quality of life in a randomized controlled trial comparing methotrexate and mycophenolate mofetil for uveitis. Ophthalmology 2021;128(9):1337-45. [CENTRAL: CN-02268128] [DOI: 10.1016/j.ophtha.2021.02.024] [PMID: ] - DOI - PMC - PubMed
-
- Kong CL, Kelly NK, Sundararajan M, Rathinam SR, Gonzales JA, Thundikandy R, et al. Comparison of CD4 counts with mycophenolate mofetil versus methotrexate from the first-line antimetabolites as steroid-sparing treatment (FAST) uveitis trial. Ocular Immunology and Inflammation 2020;30(1):1-5. [CENTRAL: CN-02161428] [DOI: 10.1080/09273948.2020.1774906] [PMID: ] - DOI - PMC - PubMed
Wiederholt 1986 {published data only}
-
- Wiederholt M, Kämpe C, Hansen LL, Hövener G. Treatment of posterior uveitis with cyclosporin or prednisolone--one-year report of a randomized prospective study [Behandlung der uveitis posterior mit cyclosporin oder prednisolon--jahresbericht über eine randomisierte prospektive studie]. Fortschritte der Ophthalmologie 1986;83(3):348‐52. [CENTRAL: CN-00044224] [EMBASE: 1986247564] [PMID: ] - PubMed
References to studies excluded from this review
BenEzra 1988 {published data only}
-
- BenEzra D, Cohen E, Chajek T, Friedman G, Pizanti S, Courten C, et al. Evaluation of conventional therapy versus cyclosporine A in Behçet's syndrome. Transplantation Proceedings 1988;20(3 Suppl 4):136‐43. [PMID: ] - PubMed
Chavis 1992 {published data only}
Masuda 1989 {published data only}
-
- Masuda K, Nakajima A, Urayama A, Nakae K, Kogure M, Inaba G. Ciclosporin treatment for Behcet's disease - double-masked group comparative study. Rinsho Hyoka [Clinical Evaluation] 1986;14:437‐61. [CENTRAL: CN-00320614]
Rosenbaum 2008 {published data only}
-
- EUCTR2006-006543-31. A double-masked, placebo-controlled, parallel group, multi-centre, dose-ranging study with an optional extension to assess the efficacy and safety of LX211 as therapy in subjects with active sight threatening, non-infectious intermediate-, anterior and intermediate-, posterior-, or pan-uveitis. who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2006-006543-31-GB (first received 09 March 2007).
-
- EUCTR2006-006544-66. A double-masked, placebo-controlled, multi-centre, parallel group, dose-ranging study to assess the efficacy and safety of LX211 as therapy in subjects with clinically quiescent sight threatening, non-infectious intermediate-, anterior and intermediate-, posterior-, or pan-uveitis. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2006-006544-66-FR (first received 06 March 2007).
-
- NCT00404612. A double-masked, placebo-controlled, parallel group, multi-centre, dose-ranging study with an optional extension to assess the efficacy and safety of LX211 as therapy in subjects with active sight threatening, non-infectious intermediate-, anterior and intermediate-, posterior-, or pan-uveitis. clinicaltrials.gov/ct2/show/NCT00404612 (first received 29 November 2006).
-
- NCT00404742. A study of LX211 in clinically quiescent non-infectious intermediate, anterior and intermediate, posterior or pan-uveitis (LUMINATE). clinicaltrials.gov/ct2/show/NCT00404742 (first received 29 November 2006).
-
- Rosenbaum JT, LUMINATE Uveitis Program Study Group. Design of phase 2/3 clinical trials of a novel calcineurin inhibitor, Lx 211, for the treatment of non-infection uveitis. Investigative Ophthalmology and Visual Science 2008;49(13):ARVO-E abstract 3883.
Shalaby 2017 {published data only}
References to studies awaiting assessment
EUCTR2006‐004709‐24‐NL {published data only (unpublished sought but not used)}
-
- EUCTR2006-004709-24-NL. Mycophenolate sodium (Myfortic®) in the treatment of uveitis: a pilot study. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2006-004709-24-NL (first received 1 September 2006).
-
- NTR1126. Myfortic in uveitis [Mycophenolate sodium (Myfortic®) in the treatment of uveitis: a pilot study]. trialsearch.who.int/?TrialID=NTR1126 (first received 2 November 2007).
JPRN‐jRCTs011180031 {published data only}
-
- JPRN-jRCTs011180031. The combination therapy of prednisolone and cyclosporine for initial onset of Vogt-Koyanagi-Harada disease [Prednisolone and cyclosporine combination therapy for early onset of Vogt-Koyanagi-Harada disease - PSL/CYA therapy for early onset of VKH disease]. www.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-jRCTs011180031 (first received 25 March 2019).
-
- UMIN000013373. The combination therapy of prednisolone and cyclosporine for initial onset of Vogt-Koyanagi-Harada disease. www.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000013373 (first received 1 April 2014).
-
- UMIN000014041. The combination therapy of prednisolone and cyclosporine for initial onset of Vogt-Koyanagi-Harada disease. www.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000014041 (first received 22 May 2014).
-
- UMIN000017093. The combination therapy of prednisolone and cyclosporine for initial onset of Vogt-Koyanagi-Harada disease. www.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000017093 (first received 10 April 2015).
UVEXATE 2017 {published data only}
-
- NCT00918554. Efficacy study of methotrexate to treat sarcoid-associated uveitis [Corticosteroid sparing effect of methotrexate in patients with sarcoid-associated uveitis: a double blind, randomized, placebo controlled-study - UVEXATE]. ClinicalTrials.gov/show/NCT00918554 (first received 11 June 2009). [CENTRAL: CN-01524320]
-
- Rodrigues F, Vicaut E, Abad S. Abortion of the UVEXATE study: are we unable to evaluate cheap and well-tolerated treatments? Clinical and Experimental Rheumatology 2017;35(1):175. [CENTRAL: CN-01338179] [EMBASE: 614510198] [PMID: ] - PubMed
Additional references
Allison 2002
Bacon 1987
Boyd 2001
Chi 2011
Chu 2017
Covidence [Computer program]
-
- Covidence. Version accessed 13 March 2022. Melbourne, Australia: Veritas Health Innovation. Available at covidence.org.
Deeks 2022
-
- Deeks JJ, Higgins JP, Altman DG, editor(s). Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook.
Dick 2013
Dick 2018
-
- Dick AD, Rosenbaum JT, Al-Dhibi HA, Belfort R Jr, Brézin AP, Fundamentals of Care for Uveitis International Consensus Group. Guidance on Noncorticosteroid Systemic Immunomodulatory Therapy in Noninfectious Uveitis: Fundamentals Of Care for UveitiS (FOCUS) Initiative. Ophthalmology 2018;125(5):757-73. [DOI: 10.1016/j.ophtha.2017.11.017] - DOI - PubMed
Durrani 2004
GetData Graph Digitizer 2.24 [Computer program]
-
- GetData Graph Digitizer 2.24. S. Fedorov, accessed 17 August 2020. Available at getdata-graph-digitizer.com.
Glanville 2006
Gómez‐Gómez 2020
-
- Gómez-Gómez A, Loza E, Rosario MP, Espinosa G, Morales JM, Spanish Society of Ocular Inflammation (SEIOC). Efficacy and safety of immunomodulatory drugs in patients with non-infectious intermediate and posterior uveitis, panuveitis and macular edema: a systematic literature review. Seminars in Arthritis and Rheumatism 2020;50(6):1299-306. [DOI: 10.1016/j.semarthrit.2020.08.010] - DOI - PubMed
GRADEpro GDT [Computer program]
-
- GRADEpro GDT. Hamilton (ON): McMaster University (developed by Evidence Prime), version accessed 3 March 2022. Available at gradepro.org.
Graffner‐Nordberg 2003
Higgins 2022a
-
- Higgins JP, Savović J, Page MJ, Elbers RG, Sterne JA. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from handbook.cochrane.org.
Higgins 2022b
-
- Higgins JP, Eldridge S, Li T, editor(s). Chapter 23: Including variants on randomized trials. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook.
Ishida 1995
Jabs 2005
-
- Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. American Journal of Ophthalmology 2005;140(3):509-16. [DOI: 10.1016/j.ajo.2005.03.057] - DOI - PMC - PubMed
Jawad 2013
Kandiel 2005
Karam 2022
-
- Karam M, Alsaif A, Al-Naseem A, Hayre A, Al Jabbouri A, Aldubaikhi A, et al. Mycophenolate versus methotrexate in non-infectious ocular inflammatory disease: a systematic review and meta-analysis. Ocular Immunology and Inflammation 2022 Feb 24 [Epub ahead of print]. [DOI: 10.1080/09273948.2022.2034166] - DOI - PubMed
Knickelbein 2017
Leal 2019
Lee 2014
Mangione 2001
-
- Mangione CM, Lee PP, Gutierrez PR, Spritzer K, Berry S, Hays RD. Development of the 25-item National Eye Institute Visual Function Questionnaire. Archives of Ophthalmology (Chicago, Ill. : 1960) 2001;119(7):1050-8. [PMID: ] - PubMed
McKenzie 2022
-
- McKenzie JE, Brennan SE, Ryan RE, Thomson HJ, Johnston RV. Chapter 9: Summarizing study characteristics and preparing for synthesis. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook.
Nussenblatt 1985
Ortiz 1998
-
- Ortiz Z, Shea B, Suarez-Almazor ME, Moher D, Wells GA, Tugwell P. The efficacy of folic acid and folinic acid in reducing methotrexate gastrointestinal toxicity in rheumatoid arthritis. A meta-analysis of randomized controlled trials. Journal of Rheumatology 1998;25(1):36-43. [PMID: ] - PubMed
Palestine 1986
Pato 2011
-
- Pato E, Muñoz-Fernández S, Francisco F, Abad MA, Maese J, Uveitis Working Group from Spanish Society of Rheumatology. Systematic review on the effectiveness of immunosuppressants and biological therapies in the treatment of autoimmune posterior uveitis. Seminars in Arthritis and Rheumatism 2011;40(4):314-23. [DOI: 10.1016/j.semarthrit.2010.05.008] - DOI - PubMed
Review Manager Web 2020 [Computer program]
-
- Review Manager Web (RevMan Web). Version 1.22.0. The Cochrane Collaboration, 2020. Available at revman.cochrane.org.
Schünemann 2022
-
- Schünemann HJ, Higgins JP, Vist GE, Glasziou P, Akl EA, Skoetz N, et al. Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook.
Sugita 2006
Tallouzi 2021
Tsirouki 2018
van Dieren 2006
-
- Van Dieren JM, Kuipers EJ, Samsom JN, Nieuwenhuis EE, Van der Woude CJ. Revisiting the immunomodulators tacrolimus, methotrexate, and mycophenolate mofetil: their mechanisms of action and role in the treatment of IBD. Inflammatory Bowel Diseases 2006;12(4):311-27. [DOI: 10.1097/01.MIB.0000209787.19952.53] - DOI - PubMed
References to other published versions of this review
Edwards Mayhew 2021
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous