

Biomechanical Phenotyping of Chronic Low Back Pain: Protocol for BACPAC
- PMID: 36315101
- PMCID: PMC10403313
- DOI: 10.1093/pm/pnac163
Biomechanical Phenotyping of Chronic Low Back Pain: Protocol for BACPAC
Abstract
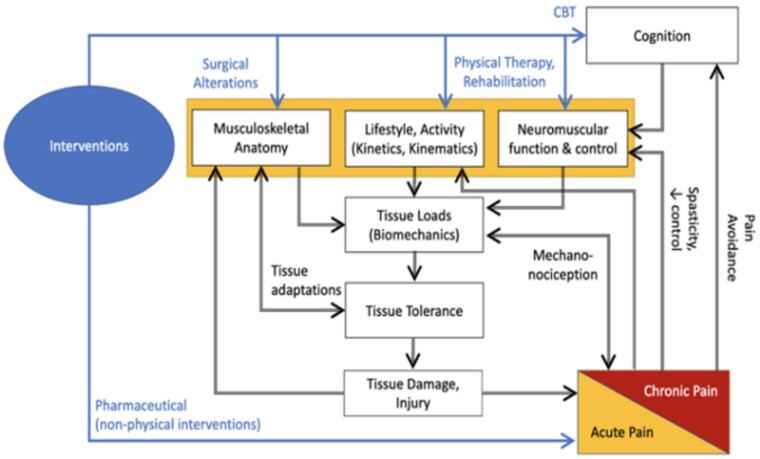
Objective: Biomechanics represents the common final output through which all biopsychosocial constructs of back pain must pass, making it a rich target for phenotyping. To exploit this feature, several sites within the NIH Back Pain Consortium (BACPAC) have developed biomechanics measurement and phenotyping tools. The overall aims of this article were to: 1) provide a narrative review of biomechanics as a phenotyping tool; 2) describe the diverse array of tools and outcome measures that exist within BACPAC; and 3) highlight how leveraging these technologies with the other data collected within BACPAC could elucidate the relationship between biomechanics and other metrics used to characterize low back pain (LBP).
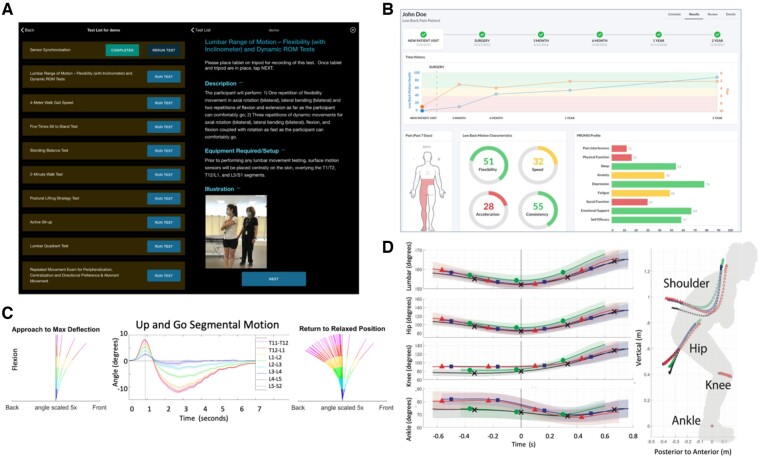
Methods: The narrative review highlights how biomechanical outcomes can discriminate between those with and without LBP, as well as among levels of severity of LBP. It also addresses how biomechanical outcomes track with functional improvements in LBP. Additionally, we present the clinical use case for biomechanical outcome measures that can be met via emerging technologies.
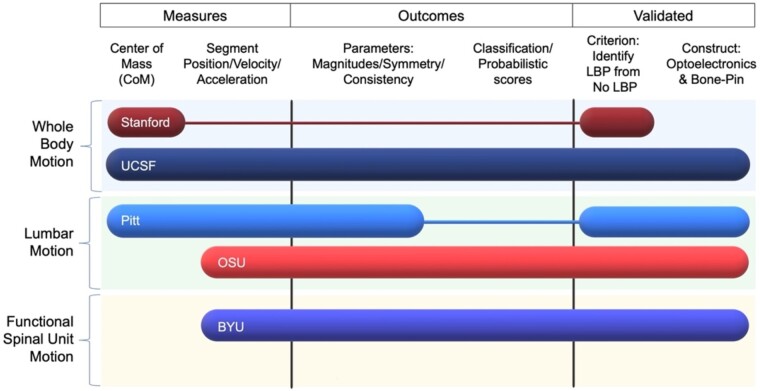
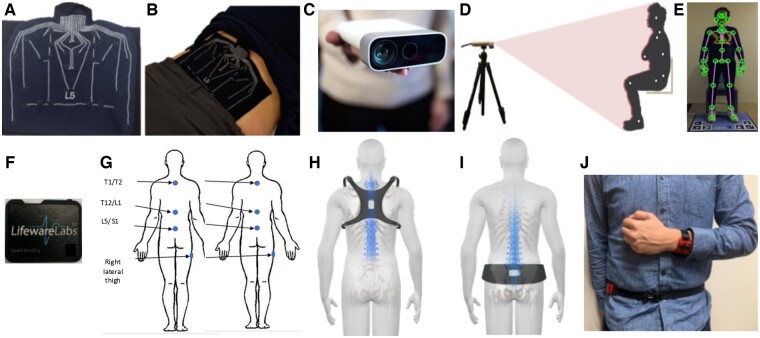
Results: To answer the need for measuring biomechanical performance, our "Results" section describes the spectrum of technologies that have been developed and are being used within BACPAC.
Conclusion and future directions: The outcome measures collected by these technologies will be an integral part of longitudinal and cross-sectional studies conducted in BACPAC. Linking these measures with other biopsychosocial data collected within BACPAC increases our potential to use biomechanics as a tool for understanding the mechanisms of LBP, phenotyping unique LBP subgroups, and matching these individuals with an appropriate treatment paradigm.
Keywords: Biomechanics; Human Movement; Low Back Disorders; Low Back Pain; Motion Analysis Technology.
© The Author(s) 2022. Published by Oxford University Press on behalf of the American Academy of Pain Medicine.
Figures
References
-
- Hoy D, March L, Brooks P, et al. The global burden of low back pain: Estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 2014;73(6):968–74. - PubMed
-
- Knezevic NN, Candido KD, Vlaeyen JWS, Zundert JV, Cohen SP.. Low back pain. Lancet 2021;398(10294):78–92. - PubMed
-
- da Silva T, Mills K, Brown BT, et al. Risk of recurrence of low back pain: A systematic review. J Orthop Sport Phys 2017;47(5):305–13. - PubMed
-
- Marras WS. The complex spine: The multidimensional system of causal pathways for low-back disorders. Hum Factors J Hum Factors Ergonom Soc 2012;54(6):881–9. - PubMed
-
- James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Lond Engl 2018;392(10159):1789–858. - PMC - PubMed
