

Effect of High-Intensity Interval Training in Patients With Atrial Fibrillation: A Randomized Clinical Trial
- PMID: 36315143
- PMCID: PMC9623436
- DOI: 10.1001/jamanetworkopen.2022.39380
Effect of High-Intensity Interval Training in Patients With Atrial Fibrillation: A Randomized Clinical Trial
Abstract
Importance: Patients with atrial fibrillation (AF) experience poor functional capacity and quality of life (QOL). High-intensity interval training (HIIT) has been shown to elicit greater improvements in functional capacity and QOL compared with moderate to vigorous intensity continuous training (MICT) in other cardiovascular populations, yet HIIT remains understudied in AF.
Objective: To compare the effects of 12 weeks of HIIT and MICT-based cardiovascular rehabilitation (CR) on functional capacity and general QOL in patients with persistent and permanent AF. Disease-specific QOL, resting heart rate (HR), time in AF, and physical activity (PA) levels were also assessed.
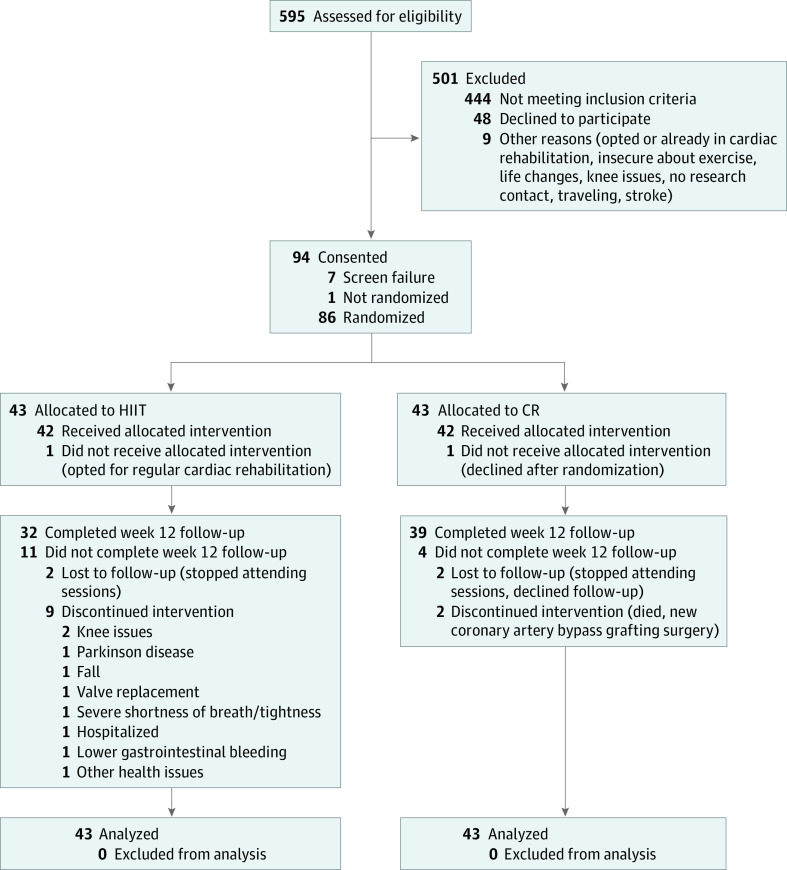
Design, setting, and participants: This randomized clinical trial, conducted between November 17, 2015, and February 4, 2020, at a tertiary-care cardiovascular health center in Ottawa, Canada, recruited 94 patients with persistent and permanent AF.
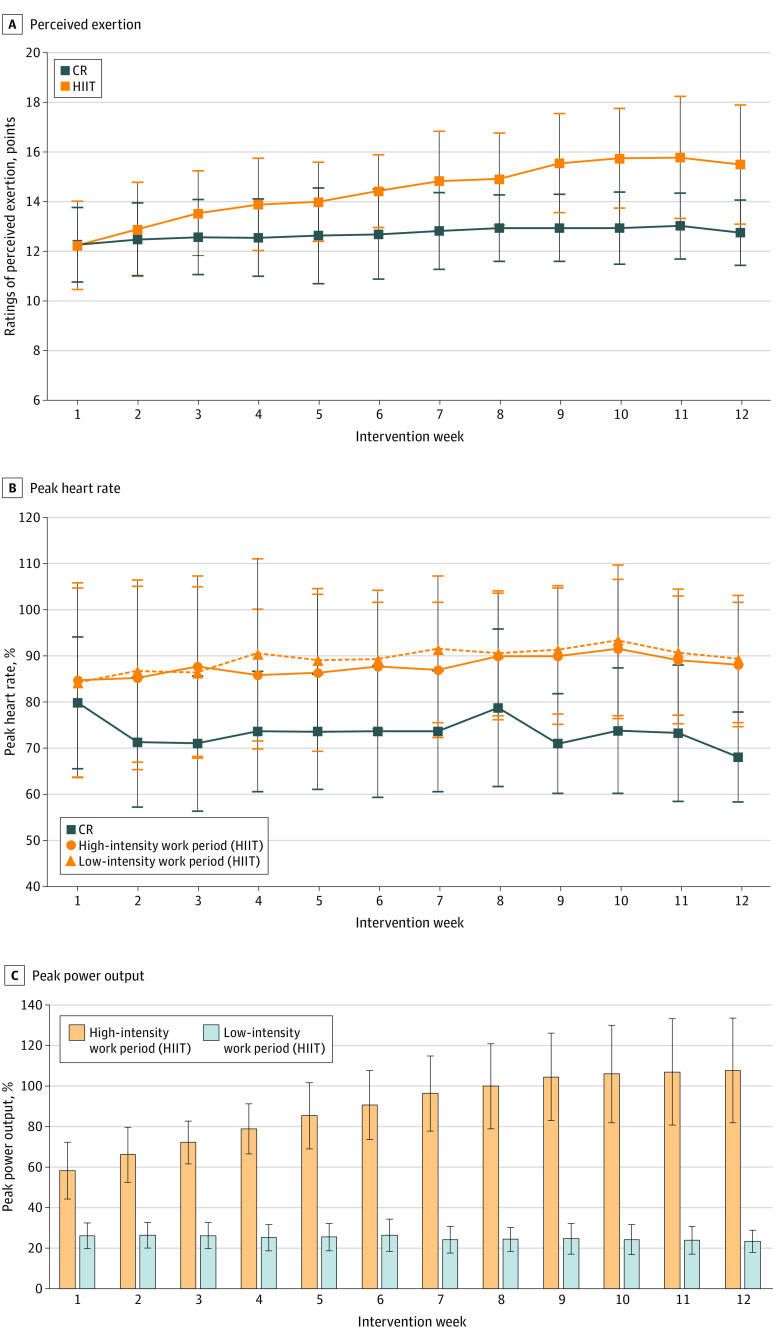
Interventions: High-intensity interval training (23 minutes: two 8-minute interval training blocks of 30-second work periods at 80%-100% of peak power output interspersed with 30-second recovery) or CR (60 minutes: continuous aerobic conditioning within 67%-95% of peak HR and 12-16 of 20 ratings of perceived exertion) twice weekly for 12 weeks.
Main outcomes and measures: The primary outcomes were changes in functional capacity (6-minute walk test [6MWT] distance) and general QOL (Short Form 36) from baseline to 12 weeks' follow-up. Secondary outcomes included changes in disease-specific QOL (Atrial Fibrillation Severity Scale), resting HR, time in AF, and PA levels. An intention-to-treat analysis was used to compare changes between groups.
Results: Of the 94 patients who consented, 86 participated (mean [SD] age, 69 [7] years; 57 [66.3%] men). No significant differences in improvements in 6MWT distance (mean [SD], 21.3 [34.1] vs 13.2 [55.2] m; P = .42) and general QOL (Physical Component Summary, 0.5 [6.1] vs 1.1 [4.9] points; P = .87) between HIIT and CR were observed. No significant differences in improvements in disease-specific QOL (AF symptoms: -1.7 [4.3] vs -1.5 [4] points, P = .59), resting HR (-3.6 [10.6] vs -2.9 [12.4] beats per minute, P = .63), and moderate to vigorous PA levels (37.3 [93.4] vs 14.4 [125.7] min/wk; P = .35) between HIIT and CR were detected. Participants attended a mean (SD) of 18.3 (6.1) (75.1%) HIIT sessions and 20.0 (4.5) (83.4%) CR sessions (P = .36).
Conclusions and relevance: In this randomized clinical trial, twice-weekly 23-minute HIIT was as efficacious as twice-weekly 60-minute CR in improving functional capacity, general and disease-specific QOL, resting HR, and PA levels in patients with persistent and permanent AF.
Trial registration: ClinicalTrials.gov Identifier: NCT02602457.
Conflict of interest statement
Figures
References
-
- Dai H, Zhang Q, Much AA, et al. . Global, regional, and national prevalence, incidence, mortality, and risk factors for atrial fibrillation, 1990-2017: results from the Global Burden of Disease Study 2017. Eur Heart J Qual Care Clin Outcomes. 2021;7(6):574-582. doi:10.1093/ehjqcco/qcaa061 - DOI - PMC - PubMed
-
- Aliot E, Breithardt G, Brugada J, et al. ; Atrial Fibrillation AWareness And Risk Education group; Atrial Fibrillation Association; European Heart Rhythm Association; Stroke Alliance for Europe; World Heart Federation . An international survey of physician and patient understanding, perception, and attitudes to atrial fibrillation and its contribution to cardiovascular disease morbidity and mortality. Europace. 2010;12(5):626-633. doi:10.1093/europace/euq109 - DOI - PMC - PubMed
-
- Smart NA, King N, Lambert JD, et al. . Exercise-based cardiac rehabilitation improves exercise capacity and health-related quality of life in people with atrial fibrillation: a systematic review and meta-analysis of randomised and non-randomised trials. Open Heart. 2018;5(2):e000880. doi:10.1136/openhrt-2018-000880 - DOI - PMC - PubMed
