

The Effect of Nitazoxanide on the Clinical Outcomes in Patients with COVID-19: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 36315350
- PMCID: PMC9628625
- DOI: 10.1007/s40261-022-01213-y
The Effect of Nitazoxanide on the Clinical Outcomes in Patients with COVID-19: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
Background and objective: Nitazoxanide, a US Food and Drug Administration-approved antiparasitic agent, was reported to be effective in treating coronavirus disease 2019 (COVID-19). The lack of effective and precise treatments for COVID-19 infection earlier in the pandemic forced us to depend on symptomatic, empirical, and supportive therapy, which overburdened intensive care units and exhausted hospital resources. Therefore, the aim of this systematic review and meta-analysis was to assess the efficacy and safety of nitazoxanide for COVID-19 treatment.
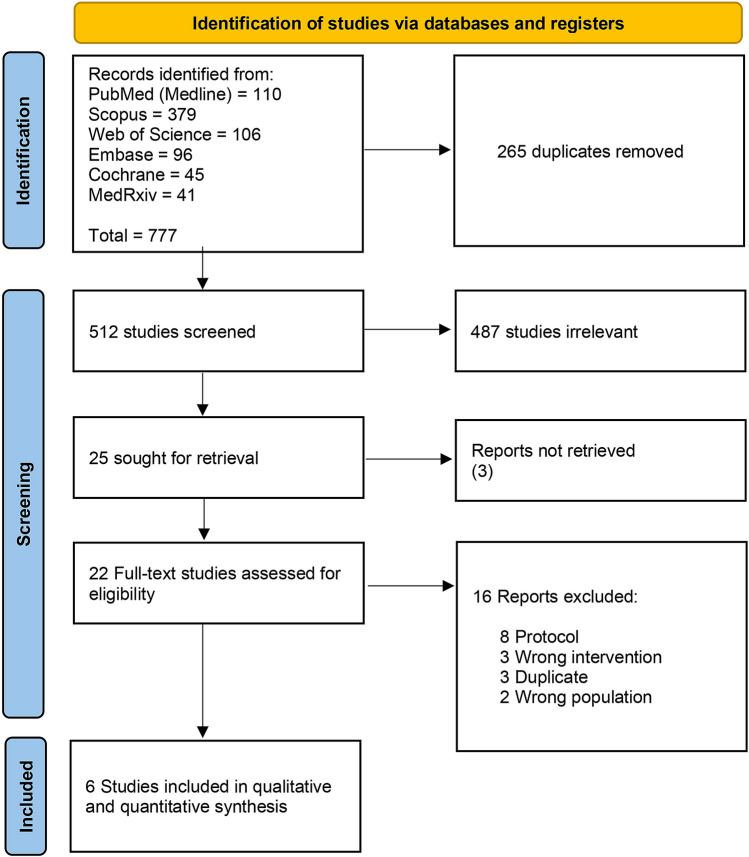
Methods: A systematic review and meta-analysis synthesizing relevant randomized controlled trials from six databases (MedRxiv, WOS, SCOPUS, EMBASE, PubMed, and CENTRAL) until 17 May 2022 was conducted. Risk ratio (RR) for dichotomous outcomes was used and data with a 95% confidence interval (CI) are presented. The protocol was registered in PROSPERO with ID: CRD42022334658.
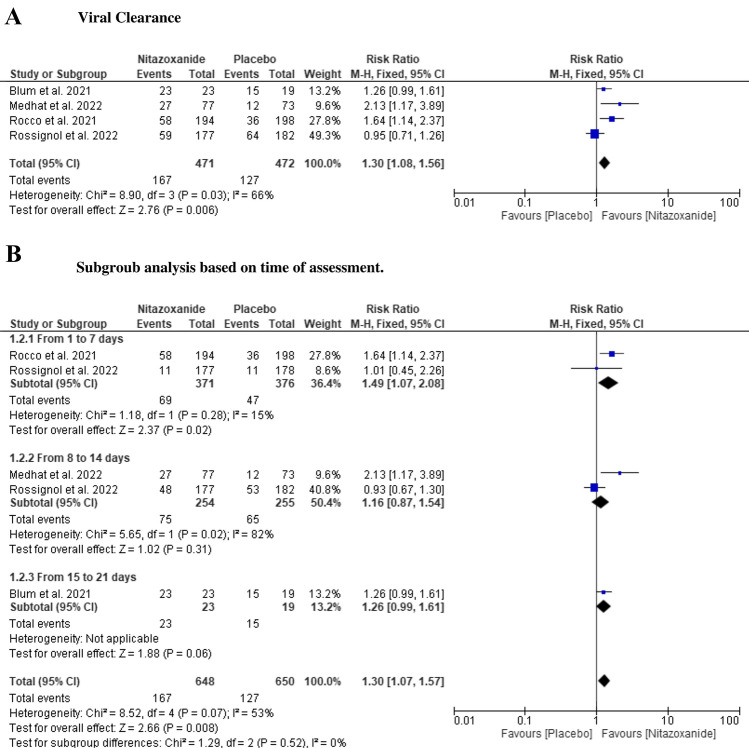
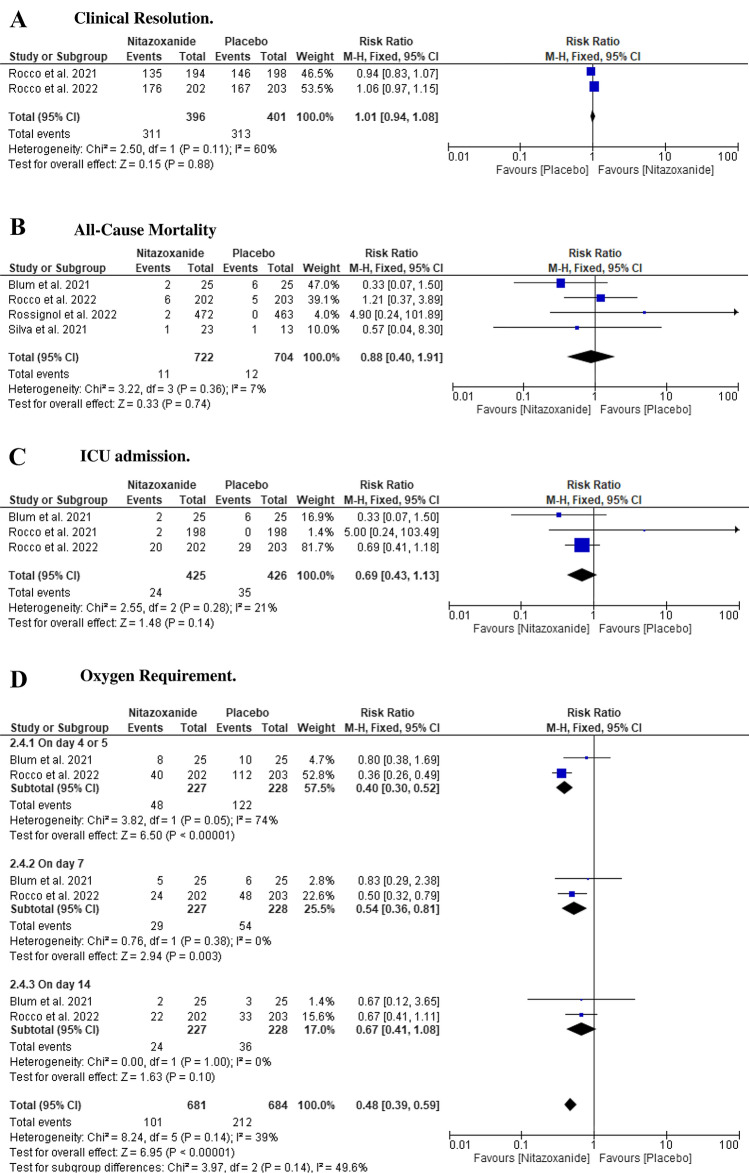
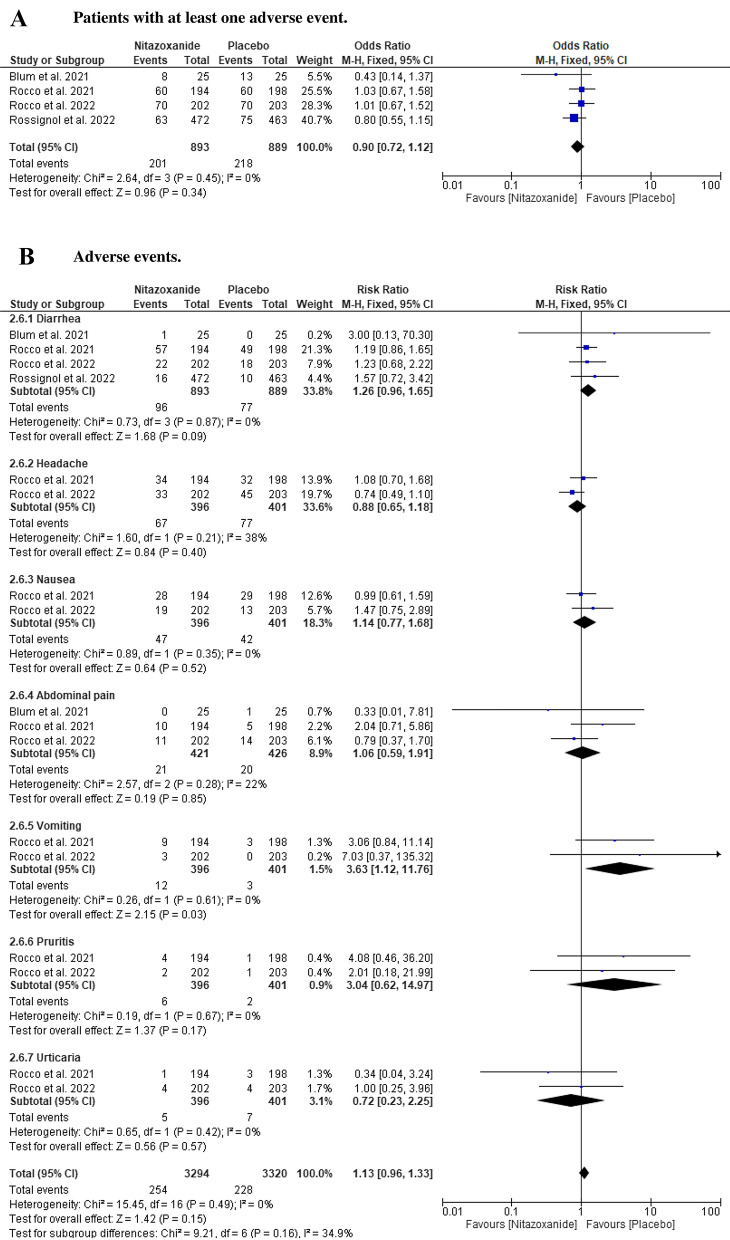
Results: Six randomized controlled trials with 1412 patients were included in the analysis. Nitazoxanide was effective in accelerating viral clearance compared with placebo (RR: 1.30 with 95% CI 1.08, 1.56, p = 0.006) and reducing oxygen requirements (RR: 0.48 with 95% CI 0.39, 0.59, p = 0.00001), but we found no difference between nitazoxanide and placebo in improving clinical resolution (RR: 1.01 with 95% CI 0.94, 1.08, p = 0.88), reducing the mortality rate (RR: 0.88 with 95% CI 0.4, 1.91, p = 0.74), and intensive care unit admission (RR: 0.69 with 95% CI 0.43, 1.13, p = 0.14). Moreover, nitazoxanide was as safe as placebo (RR: 0.9 with 95% CI 0.72, 1.12, p = 0.34).
Conclusions: Compared with placebo, nitazoxanide was effective in expediting viral clearance and decreasing oxygen requirements. However, there was no difference between nitazoxanide and placebo regarding clinical response, all-cause mortality, and intensive care unit admission. Therefore, more large-scale studies are still needed to ascertain the clinical applicability of nitazoxanide in COVID-19.
© 2022. The Author(s).
Conflict of interest statement
Mohamed Abuelazm, Ahmed Ghanem, Ahmed K. Awad, Ramadan Abdelmoez Farahat, Fatma Labieb, Basant E. Katamesh, and Basel Abdelazeem have no conflicts of interest that are directly relevant to the content of this article.
Figures

References
-
- Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, evaluation, and treatment of coronavirus (COVID-19). In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
