

Demographics of Cauda Equina Syndrome: A Population-Based Incidence Study
- PMID: 36315989
- PMCID: PMC9945186
- DOI: 10.1159/000527727
Demographics of Cauda Equina Syndrome: A Population-Based Incidence Study
Abstract
Introduction: Cauda equina syndrome (CES) has significant medical, social, and legal consequences. Understanding the number of people presenting with CES and their demographic features is essential for planning healthcare services to ensure timely and appropriate management. We aimed to establish the incidence of CES in a single country and stratify incidence by age, gender, and socioeconomic status. As no consensus clinical definition of CES exists, we compared incidence using different diagnostic criteria.
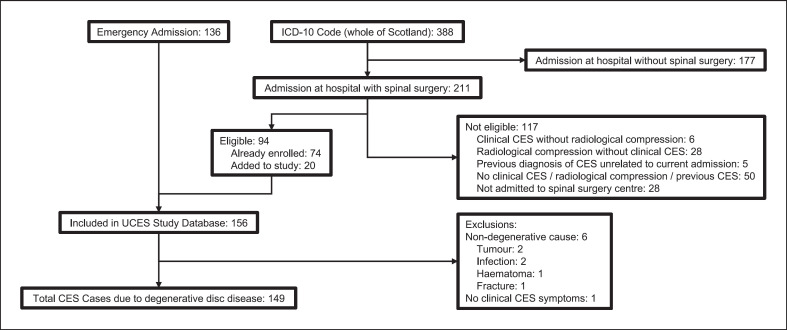
Methods: All patients presenting with radiological compression of the cauda equina due to degenerative disc disease and clinical CES requiring emergency surgical decompression during a 1-year period were identified at all centres performing emergency spinal surgery across Scotland. Initial patient identification occurred during the emergency hospital admission, and case ascertainment was checked using ICD-10 diagnostic coding. Clinical information was reviewed, and incidence rates for all demographic and clinical groups were calculated.
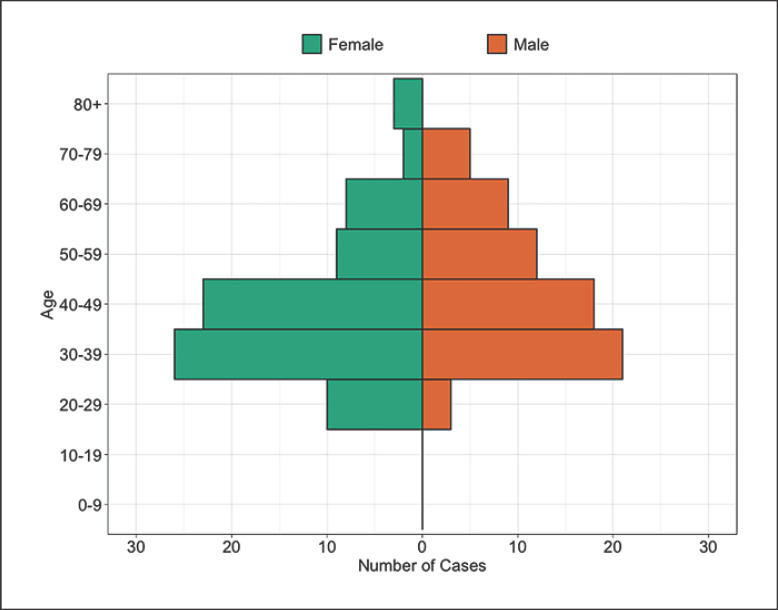
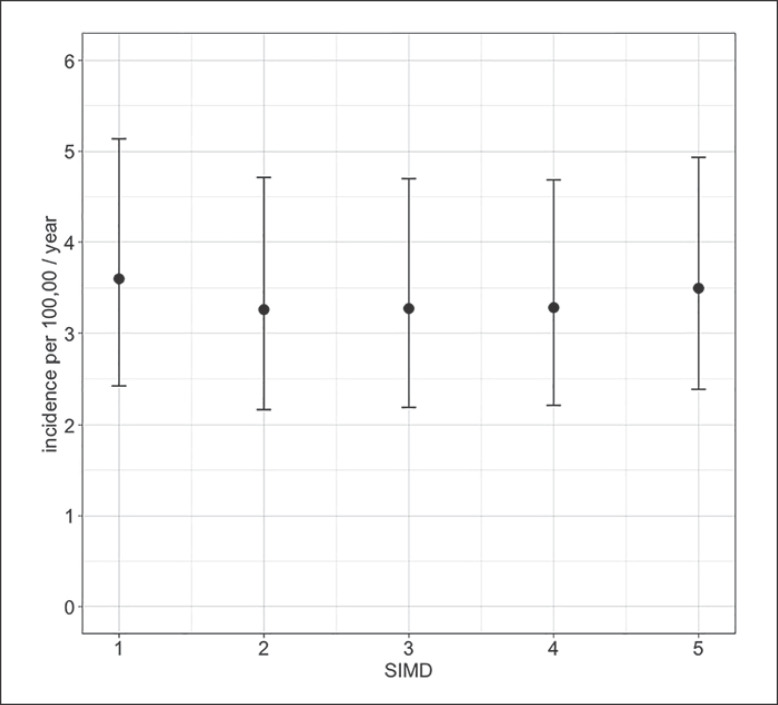
Results: We identified 149 patients with CES in 1 year from a total population of 5.4 million, giving a crude incidence of 2.7 (95% CI: 2.3-3.2) per 100,000 per year. CES occurred more commonly in females and in the 30-49 years age range, with an incidence per year of 7.2 (95% CI: 4.7-10.6) per 100,000 females age 30-39. There was no association between CES and socioeconomic status. CES requiring catheterization had an incidence of 1.1 (95% CI: 0.8-1.5) per 100,000 adults per year. The use of ICD-10 codes alone to identify cases gave much higher incidence rates, but was inaccurate, with 55% (117/211) of patients with a new ICD-10 code for CES found not to have CES on clinical notes review.
Conclusion: CES occurred more commonly in females and in those between 30 and 49 years and had no association with socioeconomic status. The incidence of CES in Scotland is at least four times higher than previous European estimates of 0.3-0.6 per 100,000 population per year. Incidence varies with clinical diagnostic criteria. To enable comparison of rates of CES across populations, we recommend using standardized clinical and radiological criteria and standardization for population structure.
Keywords: Cauda equina syndrome; Demographics; Incidence; Spine.
© 2022 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
J. Woodfield, S. Lammy, A.A.B. Jamjoom, M.A.G. Fadelalla, P.C. Copley, M. Arora, S.A. Glasmacher, M. Abdelsadg, G. Scicluna, M.T.C. Poon, S. Pronin, A.H.C. Leung, S. Darwish, J. Brown, and N. Eames have no conflicts of interest to declare. I. Hoeritzauer declares honoraria for speaking about functional neurological disorders and has received payment for expert testimony on idiopathic urinary retention. P.F.X. Statham has received payment for expert testimony, acting for a number of both claimants and defenders in cases of CES, roughly in the proportion 2/3 defender, 1/3 claimant over about 20 years. A.K. Demetriades declares payment or honoraria for speaking for Integra, Stryker, and Safe Orthopaedics and declares unpaid leadership board roles for Global Neuro Foundation and European Association of Neurosurgical Societies.
Figures
References
-
- Fraser S, Roberts L, Murphy E. Cauda equina syndrome: a literature review of its definition and clinical presentation. Arch Phys Med Rehabil. 2009 Nov;90((11)):1964–1968. - PubMed
-
- Perry S, Shaw C, Assassa P, Dallosso H, Williams K, Brittain KR, et al. An epidemiological study to establish the prevalence of urinary symptoms and felt need in the community: the Leicestershire MRC incontinence study. J Public Health Med. 2000 Sep;22((3)):427–434. - PubMed
-
- Hoy D, Brooks P, Blyth F, Buchbinder R. The Epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010 Dec;24((6)):769–781. - PubMed
-
- Reito A, Kyrola K, Pekkanen L, Paloneva J. Specific spinal pathologies in adult patients with an acute or subacute atraumatic low back pain in the emergency department. Int Orthop. 2018 May 29;42((12)):2843–2849. - PubMed
-
- Bell DA, Collie D, Statham PF. Cauda equina syndrome: what is the correlation between clinical assessment and MRI scanning? Br J Neurosurg. 2007 Apr;21((2)):201–203. - PubMed
