

Youth-onset type 2 diabetes mellitus: an urgent challenge
- PMID: 36316388
- PMCID: PMC10182876
- DOI: 10.1038/s41581-022-00645-1
Youth-onset type 2 diabetes mellitus: an urgent challenge
Abstract
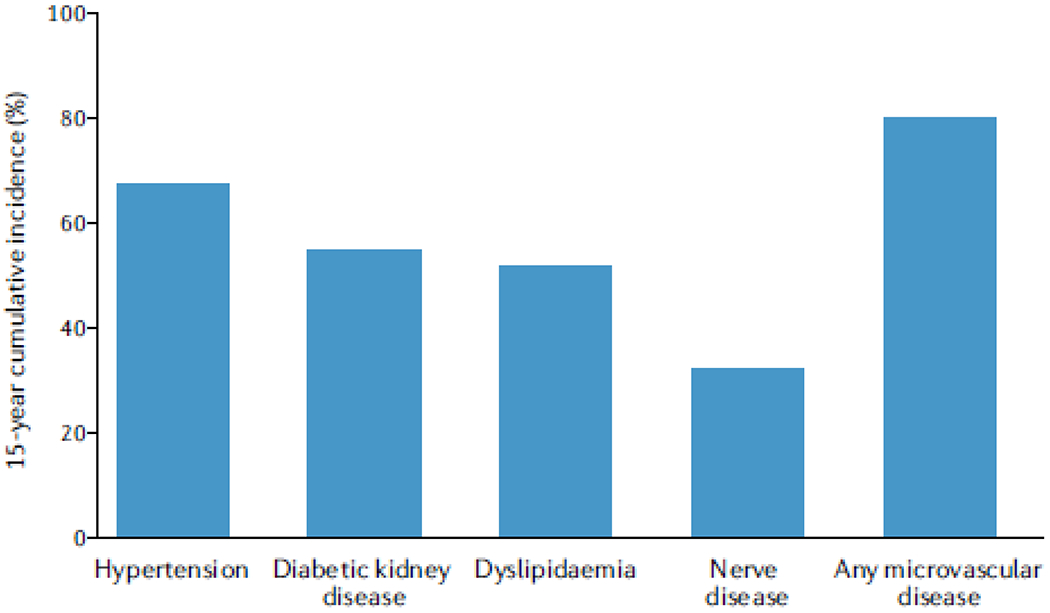
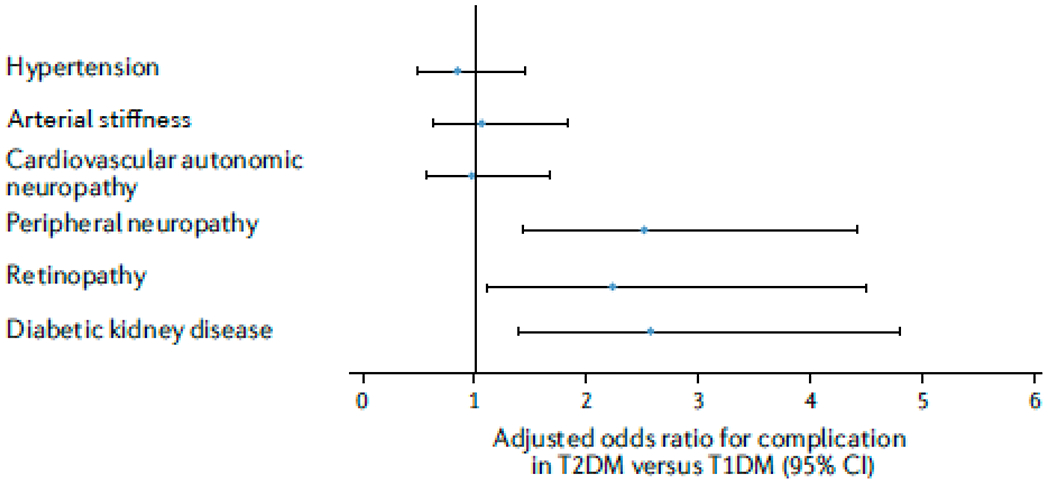
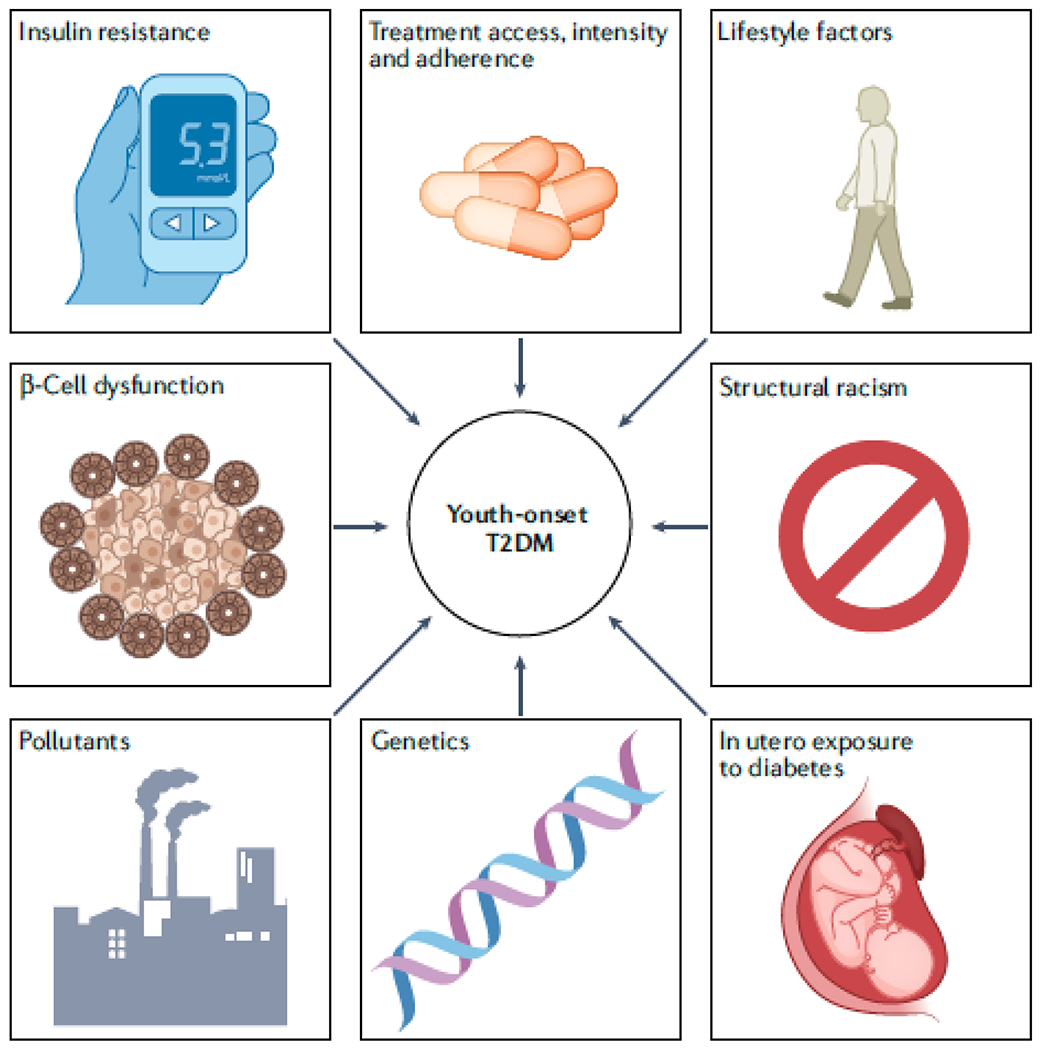
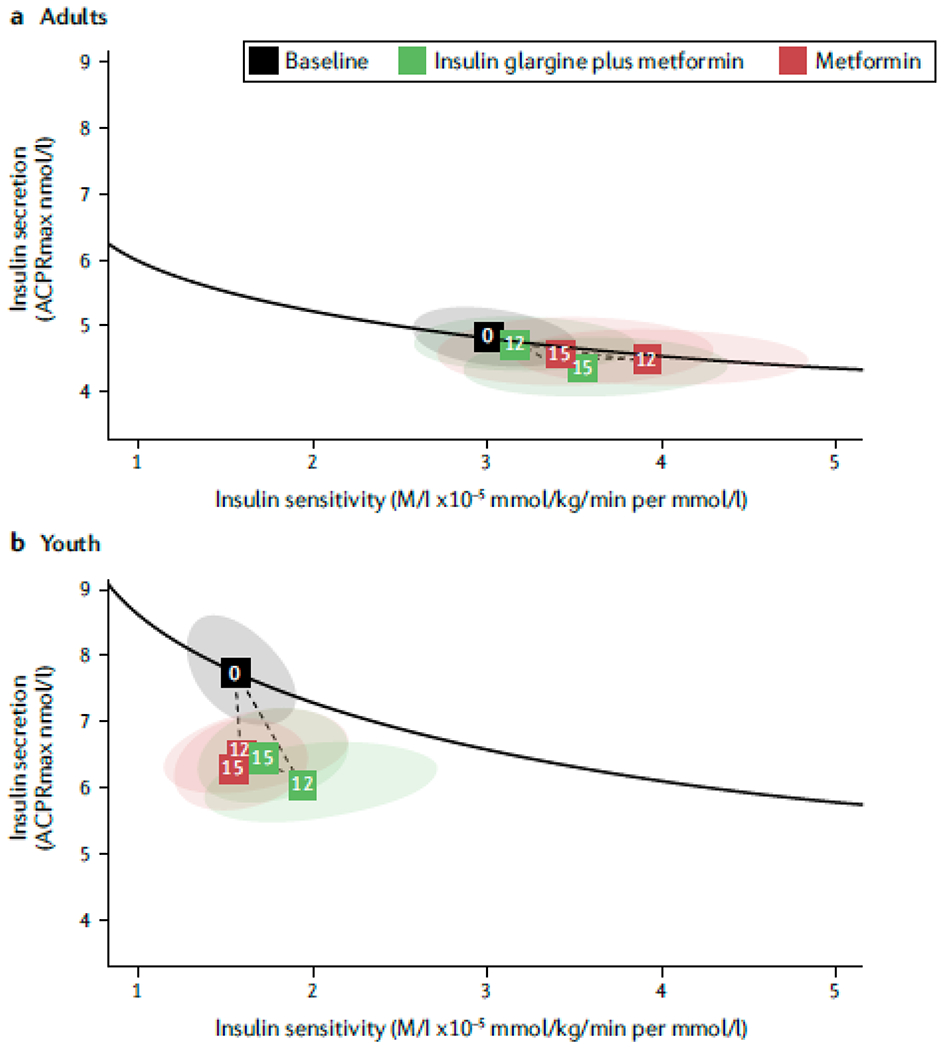
The incidence and prevalence of youth-onset type 2 diabetes mellitus (T2DM) and its complications are increasing worldwide. Youth-onset T2DM has been reported in all racial and ethnic groups, but Indigenous peoples and people of colour are disproportionately affected. People with youth-onset T2DM often have a more aggressive clinical course than those with adult-onset T2DM or those with type 1 diabetes mellitus. Moreover, the available treatment options for children and adolescents with T2DM are more limited than for adult patients. Intermediate complications of youth-onset T2DM, such as increased albuminuria, often develop in late childhood or early adulthood, and end-stage complications, including kidney failure, develop in mid-life. The increasing frequency, earlier onset and greater severity of childhood obesity in the past 50 years together with increasingly sedentary lifestyles and an increasing frequency of intrauterine exposure to diabetes are important drivers of the epidemic of youth-onset T2DM. The particularly high risk of the disease in historically disadvantaged populations suggests an important contribution of social and environmental factors, including limited access to high-quality health care, healthy food choices and opportunities for physical activity as well as exposure to stressors including systemic racism and environmental pollutants. Understanding the mechanisms that underlie the development and aggressive clinical course of youth-onset T2DM is key to identifying successful prevention and management strategies.
© 2022. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
P.B. has acted as a consultant for AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Eli-Lilly, LG Chem, Sanofi, Novo Nordisk, Horizon Pharma, XORTX. P.B. serves on the advisory boards for AstraZeneca, Bayer, Boehringer Ingelheim, Novo Nordisk and XORTX. D.H.v.R. has acted as a consultant and received honoraria from Astra Zeneca, Boehringer Ingelheim, Eli Lilly, Merck and Sanofi, and received research operating funding from AstraZeneca, Boehringer Ingelheim, Eli Lilly Diabetes Alliance and Merck. The other authors declare no competing interests.
Figures
References
-
- Fajans SS & Conn JW Tolbutamide-induced improvement in carbohydrate tolerance of young people with mild diabetes mellitus. Diabetes 9, 83–88 (1960). - PubMed
-
- Burkeholder JN, Pickens JM & Womack WN Oral glucose tolerance test in siblings of children with diabetes mellitus. Diabetes 16, 156–160 (1967). - PubMed
-
- Martin MM & Martin AL Obesity, hyperinsulinism, and diabetes mellitus in childhood. J Pediatr 82, 192–201 (1973). - PubMed
-
- Drash A Relationship between diabetes mellitus and obesity in the child. Metabolism 22, 337–344 (1973). - PubMed
-
- Deschamps I, Giron BJ & Lestradet H Blood glucose, insulin, and free fatty acid levels during oral glucose tolerance tests in 158 obese children. Diabetes 26, 89–93 (1977). - PubMed
Publication types
MeSH terms
Grants and funding
- R01 NS125316/NS/NINDS NIH HHS/United States
- P30 DK048520/DK/NIDDK NIH HHS/United States
- R01 HL165433/HL/NHLBI NIH HHS/United States
- R56 DK088971/DK/NIDDK NIH HHS/United States
- R01 HL157260/HL/NHLBI NIH HHS/United States
- R01 DK132399/DK/NIDDK NIH HHS/United States
- K23 DK116720/DK/NIDDK NIH HHS/United States
- R21 DK129720/DK/NIDDK NIH HHS/United States
- K24 HL145076/HL/NHLBI NIH HHS/United States
- U24 DK114886/DK/NIDDK NIH HHS/United States
- R01 DK119450/DK/NIDDK NIH HHS/United States
- P30 DK116073/DK/NIDDK NIH HHS/United States
- K23 RR020038/RR/NCRR NIH HHS/United States
- R01 DK129211/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
