

Potential Cardiovascular Events Avoided with Bempedoic Acid Plus Ezetimibe Fixed-Dose Combination Compared with Ezetimibe Alone in Patients with Atherosclerotic Cardiovascular Disease Taking Maximally Tolerated Statins
- PMID: 36316612
- PMCID: PMC9845167
- DOI: 10.1007/s40256-022-00552-7
Potential Cardiovascular Events Avoided with Bempedoic Acid Plus Ezetimibe Fixed-Dose Combination Compared with Ezetimibe Alone in Patients with Atherosclerotic Cardiovascular Disease Taking Maximally Tolerated Statins
Abstract
Background: Patients with atherosclerotic cardiovascular disease who require additional low-density lipoprotein cholesterol (LDL-C) lowering despite maximally tolerated statins have a significant unmet medical need and are at increased risk of future cardiovascular events and a reduced quality of life.
Objective: We aimed to estimate the percentage of cardiovascular events avoided following treatment with a fixed-dose combination of bempedoic acid plus ezetimibe (BA+EZE FDC) versus ezetimibe (EZE) in patients with atherosclerotic cardiovascular disease receiving maximally tolerated statins across a range of baseline LDL-C levels.
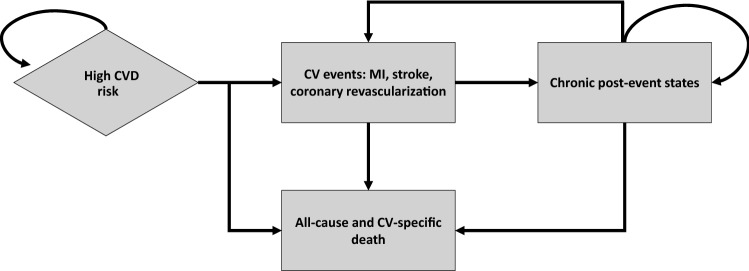
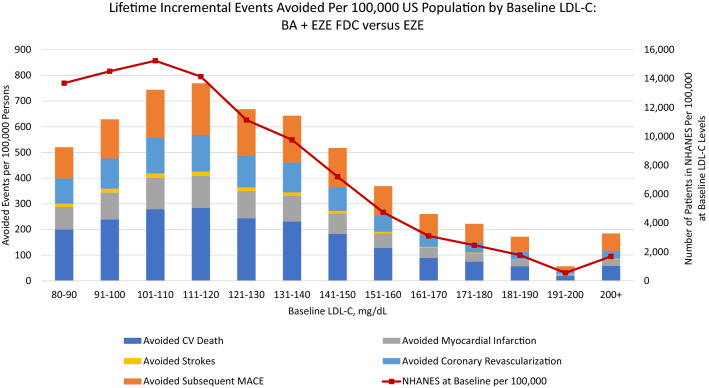
Methods: A Markov cohort simulation model estimated major adverse cardiovascular events avoided over a lifetime horizon among patients with atherosclerotic cardiovascular disease and baseline LDL-C levels from 80 to >200 mg/dL. BA+EZE FDC was compared with EZE based on mean percent LDL-C reductions versus placebo reported in a phase III trial. Health outcomes for the average patient were extrapolated to a US population of 100,000 persons using evidence on contemporary LDL-C levels from the National Health and Nutrition Examination Survey.
Results: Among patients with atherosclerotic cardiovascular disease not at the LDL-C goal with maximally tolerated statins, the addition of BA+EZE FDC compared with the addition of EZE was predicted to provide incremental absolute reductions in major adverse cardiovascular events dependent on baseline LDL-C levels at the population level. For those with baseline LDL-C of 101-110 mg/dL (n = 15,237), there were 4.9% (744) fewer events predicted, while for patients with baseline LDL-C of > 200 mg/dL (n = 1689), 10.9% (184) fewer events were predicted through the addition of BA+EZE FDC versus EZE.
Conclusions: Further LDL-C reductions through the addition of BA+EZE FDC to maximally tolerated statins are predicted to reduce major adverse cardiovascular events compared with the addition of EZE. Benefits are potentially greater among those with higher starting LDL-C.
© 2022. The Author(s).
Conflict of interest statement
R. Brett McQueen has received institutional funding to the University of Colorado from Real Endpoints, LLC. Seth J. Baum has received funding and/or consulting fees from Amgen, AstraZeneca, Axcella, Boehringer Ingelheim, Esperion, Lilly, Madrigal, and Novartis. Michael J. Louie is an employee of Esperion Therapeutics, Inc., and may own Esperion stock or stock options. William J. Sasiela is a former (retired) employee of and a current consultant for Esperion Therapeutics, Inc., and may own Esperion stock or stock options. Aikaterini Bilitou is an employee of Daiichi Sankyo Europe, GmbH, which has a corporate agreement with Esperion Therapeutics, Inc. Hemal Shah is an employee of Value Matters, LLC, and a consultant for Esperion Therapeutics, Inc. Beth Nash is a former employee and consultant of Real Endpoints, which received financial support for this study from Esperion Therapeutics, Inc. Kristin K. Gillard is an employee of Esperion Therapeutics and may own Esperion stock or stock options. Kausik K. Ray has received research grants from Amgen, Daiichi Sankyo, MSD, Pfizer, Regeneron, and Sanofi, and honoraria or consulting fees from Abbvie, Algorithm, Amgen, Astra Zeneca, Bayer, Boehringer Ingelheim, Cerenis, Cipla, Esperion, IONIS, Kowa, Lilly, Medicines Company, MSD, New Amsterdam, Novartis, Novo Nordisk, Pfizer, Regeneron, Resverlogix, Sanofi, Silence Therapeutics, and Takeda.
Figures
References
-
- World Health Organization. Cardiovascular diseases (CVDs). https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases...). Accessed 15 Feb 2019.
-
- American Heart Association. Cardiovascular disease: a costly burden for America. Projections through 2035. 2017. https://www.heart.org/-/media/files/get-involved/advocacy/burden-report-.... Accessed 15 Feb 2019.
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation. 2019;139:e1082–e1143. doi: 10.1161/CIR.0000000000000625. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
