

Incidentalomas in the head & neck
- PMID: 36317814
- PMCID: PMC9975523
- DOI: 10.1259/bjr.20220164
Incidentalomas in the head & neck
Abstract
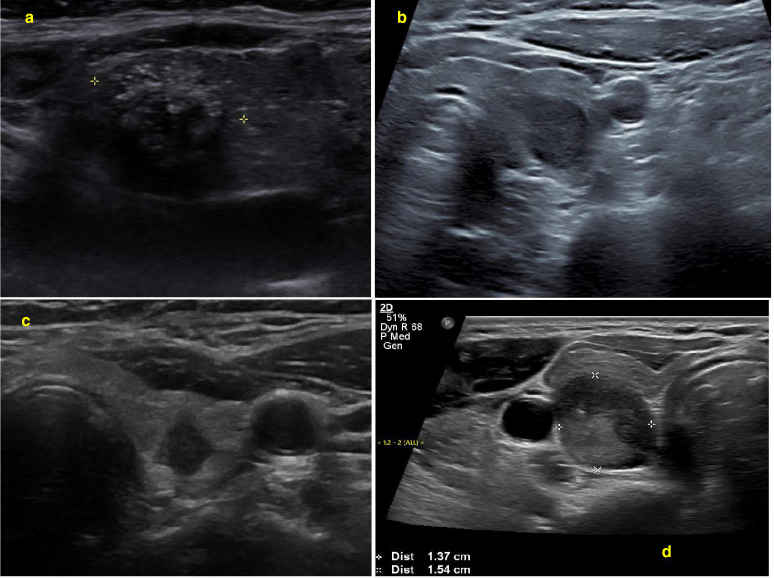
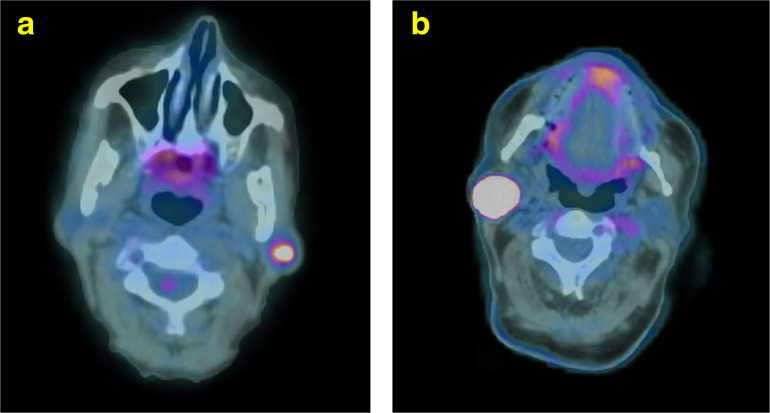
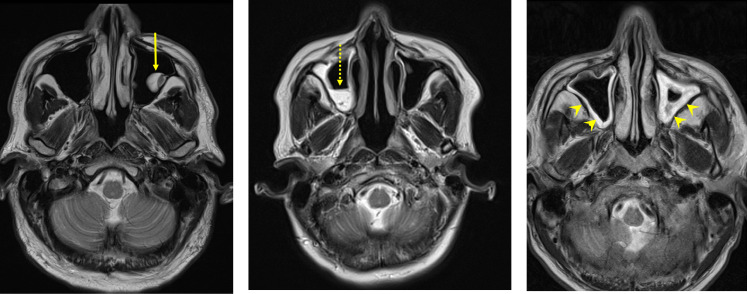
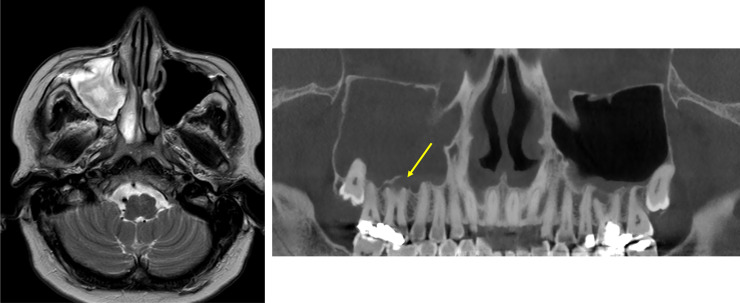
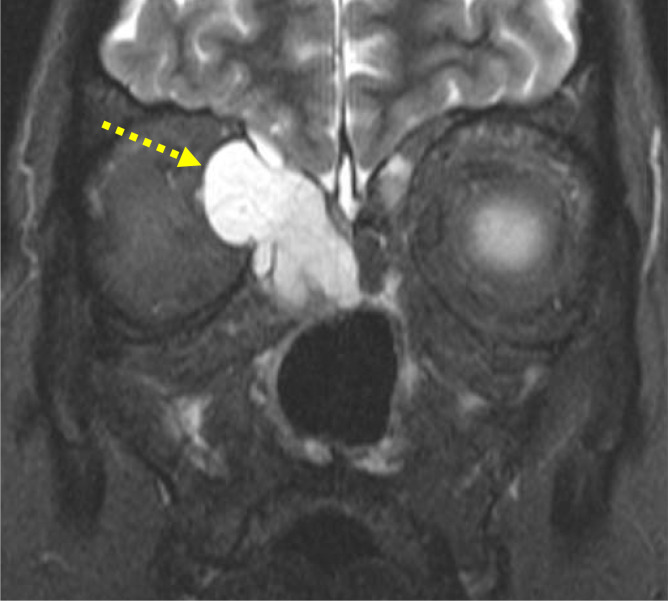
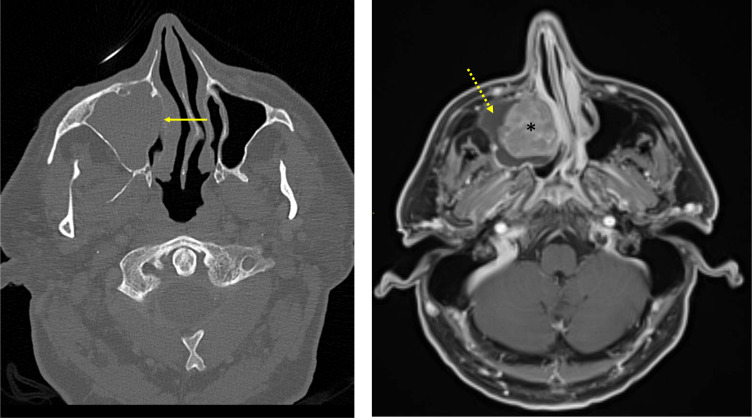
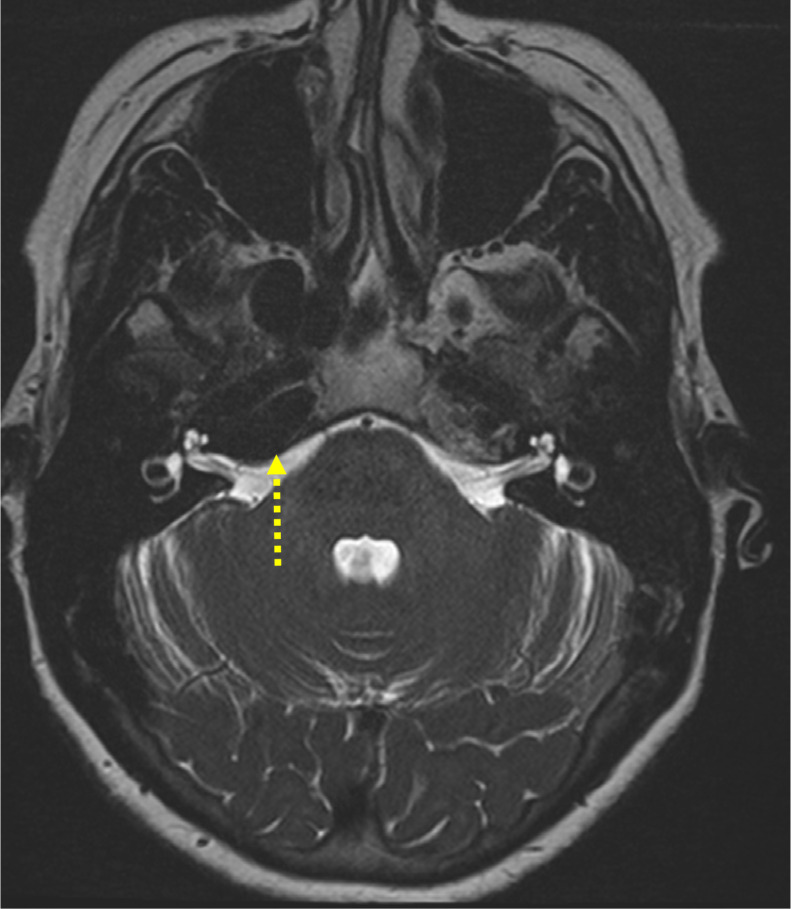
Incidental findings (IFs) in the head & neck are a frequent challenge to the reporting radiologist. A combination of complex anatomy, widely varied imaging techniques and the high prevalence of benign pathology, makes safe and appropriate management of head & neck IFs problematic. The non-head & neck radiologist is unlikely to have prior personal experience of the relevant specialties or current involvement with the pertinent multidisciplinary teams, creating unfamiliarity with both the clinical aspects of head & neck disease and the value of examination techniques. This triumvirate of complex anatomy, pathology and imaging creates the perfect environment for excessive investigation and overdiagnosis. In this article, the most frequently encountered and clinically relevant head & neck IFs are summarised. To reflect daily clinical practice, we will firstly consider anatomic abnormalities identified on cross-sectional imaging and ultrasound, followed by a review of PET-CT incidental findings.
Figures










Similar articles
-
Incidental Findings on FDG PET/CT in Head and Neck Cancer.Otolaryngol Head Neck Surg. 2018 Mar;158(3):484-488. doi: 10.1177/0194599817742579. Epub 2017 Nov 21. Otolaryngol Head Neck Surg. 2018. PMID: 29160180
-
Cross-sectional imaging in cancers of the head and neck: how we review and report.Cancer Imaging. 2016 Aug 3;16(1):20. doi: 10.1186/s40644-016-0075-3. Cancer Imaging. 2016. PMID: 27487932 Free PMC article. Review.
-
Incidental findings on 18-FDG PET-CT in head and neck cancer. A retrospective case-control study of incidental findings on 18-FDG PET-CT in patients with head and neck cancer.Eur Arch Otorhinolaryngol. 2019 Jan;276(1):243-247. doi: 10.1007/s00405-018-5203-1. Epub 2018 Dec 10. Eur Arch Otorhinolaryngol. 2019. PMID: 30535976 Free PMC article.
-
PET/CT in Head-neck Malignancies: The Implications for Personalized Clinical Practice.PET Clin. 2016 Jul;11(3):219-32. doi: 10.1016/j.cpet.2016.02.002. PET Clin. 2016. PMID: 27321027 Review.
-
Atypical 18F-FDG PET-CT uptake in the head and neck; a case-based pictorial review.Clin Imaging. 2018 May-Jun;49:136-143. doi: 10.1016/j.clinimag.2018.01.006. Epub 2018 Jan 10. Clin Imaging. 2018. PMID: 29414508 Review.
Cited by
-
Incidental imaging findings from head to toe: challenges and management: introductory editorial.Br J Radiol. 2023 Feb;96(1142):20239002. doi: 10.1259/bjr.20239002. Br J Radiol. 2023. PMID: 36692871 Free PMC article. No abstract available.
-
Definitions of Incidental [18F]FDG PET/CT Findings in the Literature: A Systematic Review and Definition Proposal.Diagnostics (Basel). 2024 Dec 9;14(23):2764. doi: 10.3390/diagnostics14232764. Diagnostics (Basel). 2024. PMID: 39682672 Free PMC article. Review.
References
-
- Grogan RH, Aschebrook-Kilfoy B, White MG, Kaplan EL, Angelos P. Thyroid incidentalomas and the overdiagnosis conundrum. International Journal of Endocrine Oncology 2016; 3: 193–96. doi: 10.2217/ije-2016-0008 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
