

Optimizing Neurodevelopmental Outcomes in Neonates With Congenital Heart Disease
- PMID: 36317967
- PMCID: PMC10435013
- DOI: 10.1542/peds.2022-056415L
Optimizing Neurodevelopmental Outcomes in Neonates With Congenital Heart Disease
Abstract
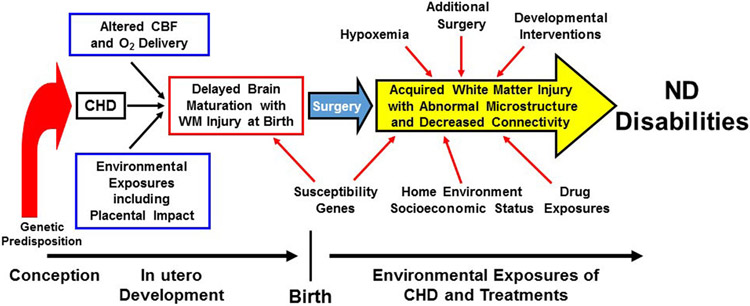
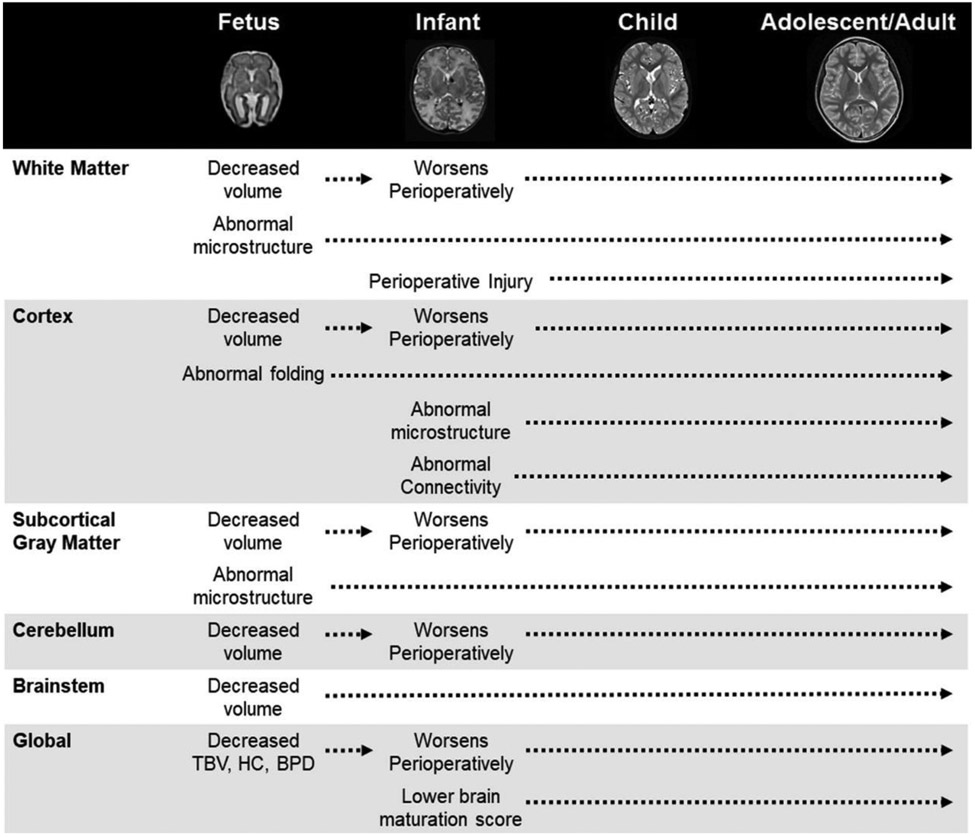
Neurodevelopmental impairment is a common and important long-term morbidity among infants with congenital heart disease (CHD). More than half of those with complex CHD will demonstrate some form of neurodevelopmental, neurocognitive, and/or psychosocial dysfunction requiring specialized care and impacting long-term quality of life. Preventing brain injury and treating long-term neurologic sequelae in this high-risk clinical population is imperative for improving neurodevelopmental and psychosocial outcomes. Thus, cardiac neurodevelopmental care is now at the forefront of clinical and research efforts. Initial research primarily focused on neurocritical care and operative strategies to mitigate brain injury. As the field has evolved, investigations have shifted to understanding the prenatal, genetic, and environmental contributions to impaired neurodevelopment. This article summarizes the recent literature detailing the brain abnormalities affecting neurodevelopment in children with CHD, the impact of genetics on neurodevelopmental outcomes, and the best practices for neonatal neurocritical care, focusing on developmental care and parental support as new areas of importance. A framework is also provided for the infrastructure and resources needed to support CHD families across the continuum of care settings.
Copyright © 2022 by the American Academy of Pediatrics.
Conflict of interest statement
Conflict of Interest:
The authors have no conflicts of interest relevant to this article to disclose.
Figures
References
-
- Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N and Kaouache M. Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation. 2014;130:749–56. - PubMed
-
- Marino BS, Lipkin PH, Newburger JW, Peacock G, Gerdes M, Gaynor JW, Mussatto KA, Uzark K, Goldberg CS, Johnson WH Jr., Li J, Smith SE, Bellinger DC, Mahle WT, American Heart Association Congenital Heart Defects Committee CoCDitYCoCN and Stroke C. Neurodevelopmental outcomes in children with congenital heart disease: evaluation and management: a scientific statement from the American Heart Association. Circulation. 2012;126:1143–72. - PubMed
-
- Bellinger DC, Jonas RA, Rappaport LA, Wypij D, Wernovsky G, Kuban KC, Barnes PD, Holmes GL, Hickey PR, Strand RD and et al. Developmental and neurologic status of children after heart surgery with hypothermic circulatory arrest or low-flow cardiopulmonary bypass. N Engl J Med. 1995;332:549–55. - PubMed
-
- Marino BS, Tomlinson RS, Wernovsky G, Drotar D, Newburger JW, Mahony L, Mussatto K, Tong E, Cohen M, Andersen C, Shera D, Khoury PR, Wray J, Gaynor JW, Helfaer MA, Kazak AE, Shea JA and Pediatric Cardiac Quality of Life Inventory Testing Study C. Validation of the pediatric cardiac quality of life inventory. Pediatrics. 2010;126:498–508. - PMC - PubMed
-
- Wray J, Brown K, Franklin R, Cassedy A and Marino BS. Assessing the generalisability of the pediatric cardiac quality of life inventory in the United Kingdom. Cardiol Young. 2014;24:220–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
