

Effectiveness of Shared Decision-making Training Programs for Health Care Professionals Using Reflexivity Strategies: Secondary Analysis of a Systematic Review
- PMID: 36318726
- PMCID: PMC9773026
- DOI: 10.2196/42033
Effectiveness of Shared Decision-making Training Programs for Health Care Professionals Using Reflexivity Strategies: Secondary Analysis of a Systematic Review
Abstract
Background: Shared decision-making (SDM) leads to better health care processes through collaboration between health care professionals and patients. Training is recognized as a promising intervention to foster SDM by health care professionals. However, the most effective training type is still unclear. Reflexivity is an exercise that leads health care professionals to question their own values to better consider patient values and support patients while least influencing their decisions. Training that uses reflexivity strategies could motivate them to engage in SDM and be more open to diversity.
Objective: In this secondary analysis of a 2018 Cochrane review of interventions for improving SDM by health care professionals, we aimed to identify SDM training programs that included reflexivity strategies and were assessed as effective. In addition, we aimed to explore whether further factors can be associated with or enhance their effectiveness.
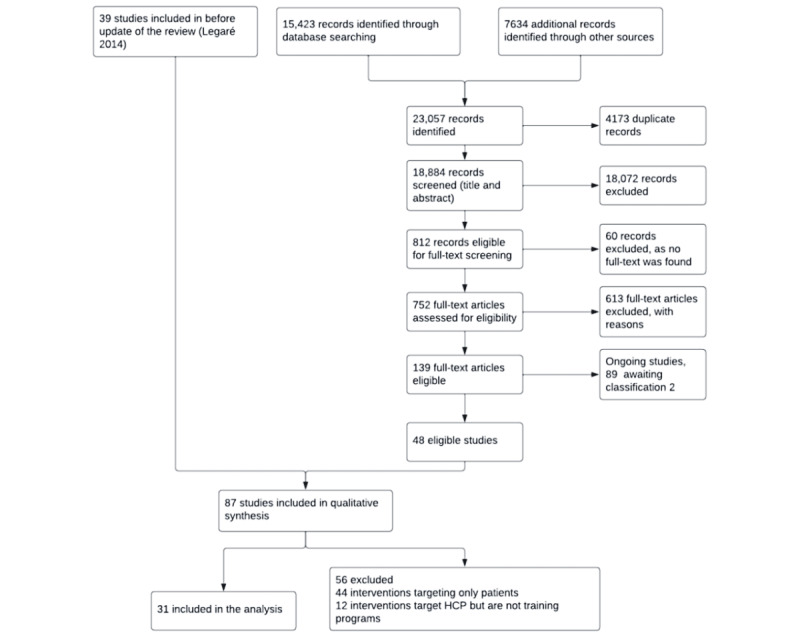
Methods: From the Cochrane review, we first extracted training programs targeting health care professionals. Second, we developed a grid to help identify training programs that used reflexivity strategies. Third, those identified were further categorized according to the type of strategy used. At each step, we identified the proportion of programs that were classified as effective by the Cochrane review (2018) so that we could compare their effectiveness. In addition, we wanted to see whether effectiveness was similar between programs using peer-to-peer group learning and those with an interprofessional orientation. Finally, the Cochrane review selected programs that were evaluated using patient-reported or observer-reported outcome measurements. We examined which of these measurements was most often used in effective training programs.
Results: Of the 31 training programs extracted, 24 (77%) were interactive, among which 10 (42%) were considered effective. Of these 31 programs, 7 (23%) were unidirectional, among which 1 (14%) was considered effective. Of the 24 interactive programs, 7 (29%) included reflexivity strategies. Of the 7 training programs with reflexivity strategies, 5 (71%) used a peer-to-peer group learning strategy, among which 3 (60%) were effective; the other 2 (29%) used a self-appraisal individual learning strategy, neither of which was effective. Of the 31 training programs extracted, 5 (16%) programs had an interprofessional orientation, among which 3 (60%) were effective; the remaining 26 (84%) of the 31 programs were without interprofessional orientation, among which 8 (31%) were effective. Finally, 12 (39%) of 31 programs used observer-based measurements, among which more than half (7/12, 58%) were effective.
Conclusions: Our study is the first to evaluate the effectiveness of SDM training programs that include reflexivity strategies. Its conclusions open avenues for enriching future SDM training programs with reflexivity strategies. The grid developed to identify training programs that used reflexivity strategies, when further tested and validated, can guide future assessments of reflexivity components in SDM training.
Keywords: health care professionals; implementation; reflexivity; shared decision-making; training.
©Ndeye Thiab Diouf, Angèle Musabyimana, Virginie Blanchette, Johanie Lépine, Sabrina Guay-Bélanger, Marie-Claude Tremblay, Maman Joyce Dogba, France Légaré. Originally published in JMIR Medical Education (https://mededu.jmir.org), 07.12.2022.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Shay LA, Lafata JE. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med Decis Making. 2015 Jan;35(1):114–31. doi: 10.1177/0272989X14551638. https://europepmc.org/abstract/MED/25351843 0272989X14551638 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
